0001429560
false
0001429560
2023-09-06
2023-09-06
iso4217:USD
xbrli:shares
iso4217:USD
xbrli:shares
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported):
September 6, 2023
TREVENA, INC.
(Exact name of registrant as specified in
its charter)
Delaware
(State or other jurisdiction of incorporation)
| 001-36193 |
|
26-1469215 |
(Commission
File No.) |
|
(IRS Employer
Identification No.) |
955 Chesterbrook Boulevard, Suite 110
Chesterbrook, PA 19087
(Address of principal executive offices and zip
code)
Registrant’s telephone number, including
area code: (610) 354-8840
Not applicable
(Former name or former address, if changed
since last report.)
Check the appropriate box below if the Form 8-K filing is intended
to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ¨ | Written communications pursuant to Rule 425 under the
Securities Act (17 CFR 230.425) |
| ¨ | Soliciting material pursuant to Rule 14a-12 under the
Exchange Act (17 CFR 240.14a-12) |
| ¨ | Pre-commencement communications pursuant to Rule 14d-2(b)
under the Exchange Act (17 CFR 240.14d-2(b)) |
| ¨ | Pre-commencement communications pursuant to Rule 13e-4(c)
under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section
12(b) of the Act:
| Title of each class | |
Trading Symbol(s) | |
Name of each exchange on which registered |
| Common Stock, $0.001 par value | |
TRVN | |
The Nasdaq Stock Market LLC |
Indicate
by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405
of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter). Emerging growth company
¨
If
an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for
complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
| Item 7.01 |
Regulation FD Disclosure |
On September 6, 2023,
Trevena, Inc. (the “Company”) updated its website to include an updated corporate presentation deck. A copy of the updated
corporate deck is attached hereto as Exhibit 99.1.
Also on September 6,
2023, the Company updated its website to include a revised TRV045 overview deck. A copy of the TRV045 overview deck is attached hereto
as Exhibit 99.2.
The information set forth
on this Item 7.01 and furnished hereto as Exhibits 99.1 and 99.2 shall not be deemed “filed” for purposes of Section 18 of
the Exchange Act, and is not incorporated by reference into any of the Company’s filings under the Securities Act or the Exchange
Act, whether made before or after the date hereof, except as shall be expressly set forth by specific reference in any such filing.
On September 6, 2023, Trevena, Inc. (the “Company”) issued
two press releases. The first press release announced new preliminary data from the two Phase 1 proof-of-concept studies of TRV045. TRV045
is a novel sphingosine-1-phosphate receptor modulator selective for the S1P receptor subtype 1. The first study was the Target
Engagement (PainCart®) proof-of-concept study, and the second study was the TMS proof-of-concept study. A copy of the first press
release with more detail about both studies is furnished hereto as Exhibit 99.3 and incorporated herein by reference.
The Company’s second press release announced, among other things,
receipt of the $15 million tranche from its non-dilutive financing with R-Bridge Investment Four
Pte. Ltd., an affiliate of CBC Group, as well as other general business updates. A copy of the second press release is furnished
hereto as Exhibit 99.4 and incorporated herein by reference.
The information set forth in this Item 8.01 and furnished hereto as
Exhibit 99.3 and 99.4 shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended
(the “Exchange Act”), or incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange
Act, whether made before or after the date of this Current Report, except as shall be expressly set forth by specific reference in such
a filing.
| Item 9.01. | Financial Statements and Exhibits. |
SIGNATURES
Pursuant to the requirements of the Securities
Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| |
TREVENA, INC. |
| |
|
| Date: September 6, 2023 |
By: |
/s/ Barry Shin |
| |
|
Barry Shin |
| |
|
Senior Vice President & Chief Financial Officer |
Exhibit 99.1

INNOVATING FOR PATIENTS Nasdaq: TRVN I September 2023

Forward - Looking Statements To the extent that statements contained in this presentation are not descriptions of historical facts regarding Trevena, Inc. (t he “Company” or “we”), they are forward - looking statements reflecting management’s current beliefs and expectations. Forward - looking statements are subject to known and unknown risks, unc ertainties, and other factors that may cause our or our industry’s actual results, levels of activity, performance, or achievements to be materially different from those anticipated by such statements. You can identify forward - looking statements by terminology such as “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “might,” “plan,” “objective,” “predict,” “pr oject,” “suggest,” “target,” “potential,” “will,” “would,” “could,” “should,” “continue,” “ongoing,” or the negative of these terms or similar expressions. Forward - looking statements contained in this prese ntation include, but are not limited to, ( i ) statements regarding the timing of anticipated clinical trials for our product candidates; (ii) the timing of receipt of clinical data for our pro duc t candidates; (iii) our expectations regarding the potential safety, efficacy, or clinical utility of our product candidates; (iv) the size of patient populations targeted by our product candidates and ma rke t adoption of our potential drugs by physicians and patients; (v) the timing or likelihood of regulatory filings and approvals; and (vi) our cash needs. Actual results may differ materially from those indicated by such forward - looking statements as a result of various important f actors, including: the commercialization of any approved drug product, the status, timing, costs, results and interpretation of our clinical trials or any future trials of any of our inve sti gational drug candidates; the uncertainties inherent in conducting clinical trials; expectations for regulatory interactions, submissions and approvals, including our assessment of the discussions with th e FDA or other regulatory agencies about any and all of our programs; uncertainties related to the commercialization of OLINVYK; available funding; uncertainties related to our intellec tua l property; other matters that could affect the availability or commercial potential of our therapeutic candidates; and other factors discussed in the Risk Factors set forth in our Annual R epo rt on Form 10 - K and Quarterly Reports on Form 10 - Q filed with the Securities and Exchange Commission (SEC) and in other filings we make with the SEC from time to time. In addition, the fo rwa rd - looking statements included in this presentation represent our views only as of the date hereof. We anticipate that subsequent events and developments may cause our views to cha nge. However, while we may elect to update these forward - looking statements at some point in the future, we specifically disclaim any obligation to do so, except as may be requi red by law. 2

BOARD OF DIRECTORS Leon O. Moulder , Jr. Chairman Marvin H. Johnson, Jr. Carrie L. Bourdow Jake R. Nunn Scott Braunstein, M.D. Anne M. Phillips, M.D. Mark Corrigan, M.D. Barbara Yanni Michael R. Dougherty SENIOR MANAGEMENT Carrie L. Bourdow President & Chief Executive Officer Mark A. Demitrack , M.D . SVP, Chief Medical Officer Patricia Drake SVP, Chief Commercial Officer Barry Shin SVP, Chief Financial Officer Robert T. Yoder SVP, Chief Business Officer & Head of Commercial Operations Trevena’s Experienced Leadership Team 3
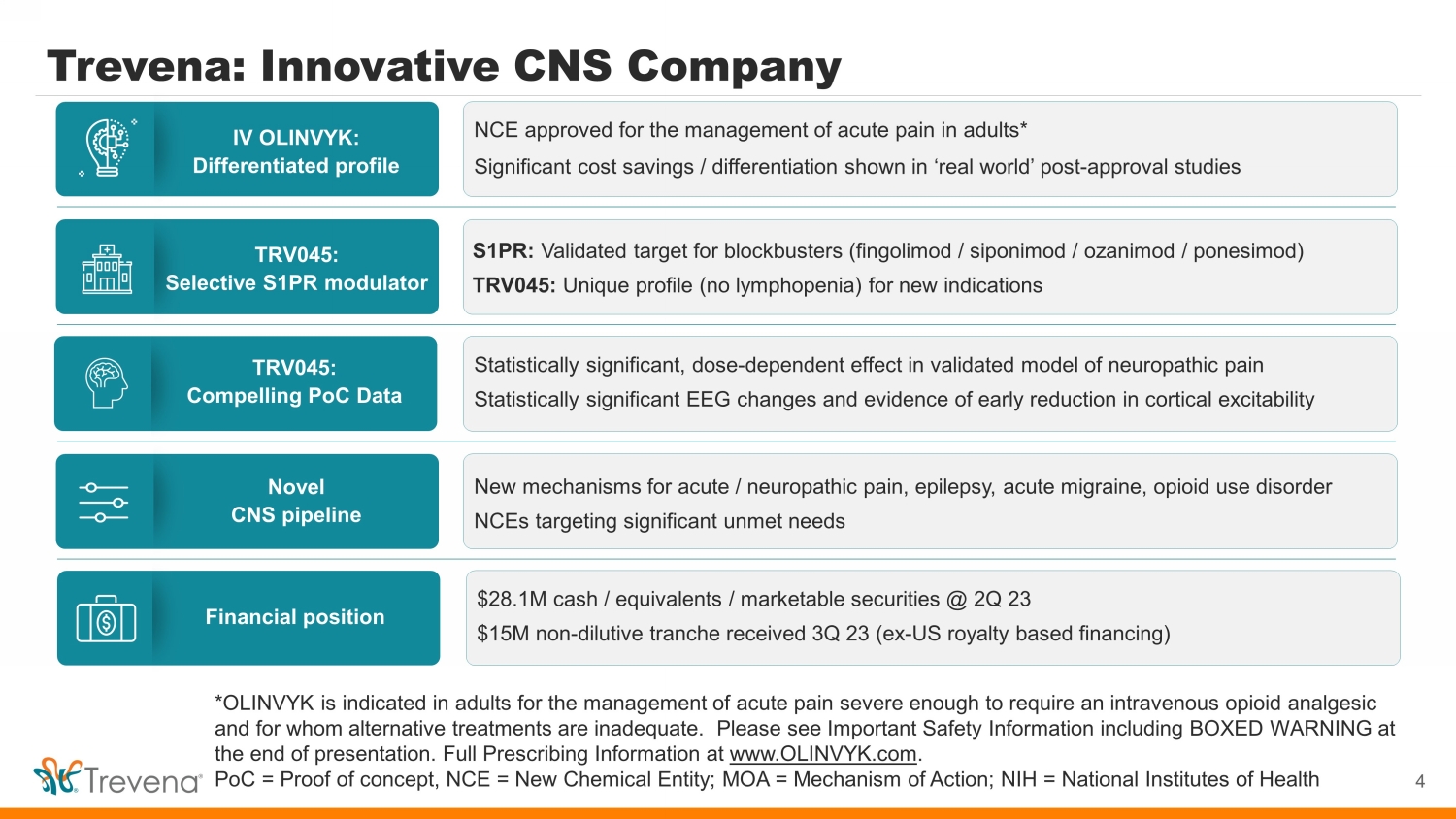
Trevena: Innovative CNS Company 4 *OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . PoC = Proof of concept, NCE = New Chemical Entity; MOA = Mechanism of Action; NIH = National Institutes of Health IV OLINVYK: Differentiated profile TRV045: Selective S1PR modulator Novel CNS pipeline TRV045: Compelling PoC Data Financial position NCE approved for the management of acute pain in adults* Significant cost savings / differentiation shown in ‘real world’ post - approval studies S1PR: Validated target for blockbusters (fingolimod / siponimod / ozanimod / ponesimod ) TRV045: Unique profile (no lymphopenia) for new indications New mechanisms for acute / neuropathic pain, epilepsy, acute migraine, opioid use disorder NCEs targeting significant unmet needs Statistically significant, dose - dependent effect in validated model of neuropathic pain Statistically significant EEG changes and e vidence of early reduction in cortical excitability $28.1M cash / equivalents / marketable securities @ 2Q 23 $15M non - dilutive tranche received 3Q 23 (ex - US royalty based financing)

PRE - CLIN PHASE 1 PHASE 2 PHASE 3 NDA POST - APPR Highlights OLINVYK® New chemical entity (mu - opioid receptor) TRV045 Selective S1P receptor modulator • Data reported • Data reported • Data expected 2H 23 TRV734 G - protein selective agonist (mu - opioid receptor) Multiple Expected Catalysts 5 NIH / NIDA collab. IV OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. * Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com. TRV045 and TRV734 are investigational products and are not approved by the FDA or any other regulatory agency NDA = New Drug Application, PoC = Proof - of - Concept, DNP = Diabetic Neuropathic Pain IV acute pain* VOLITION clinical outcomes Respiratory physiology Cleveland Clinic / Wake Forest Baptist Health collab. PoC – pain / target engagement PoC – TMS APPROVED • Real world differentiation • Data reported • Commercial launch ongoing • POC study ongoing ARTEMIS clinical outcomes • $8.8k / 1.4 day savings Opioid use disorder Seiz . Prev NIH / ETSP investigating potential disease modifying role Cognitive function Cleveland Clinic / Wake Forest Baptist Health collab. • Data reported

Ex - US Royalty - Based Financing Highlights Blue Chip Investor R - Bridge Healthcare Fund affiliate of CBC Group (one of the largest and most active healthcare - dedicated investment firms in Asia) $40M Total Financing $15M upfront $15M on first commercial sale in China $10M on commercial or financing milestone $40M total Flexible Payments* • Chinese Royalties. All royalties from Nhwa partnership, TRVN retains milestones • Capped US Royalty. 4% royalty on US OLINVYK net sales, with $10M cap Constructive Terms • No financial covenants 6 Received 3Q 23

OLINVYK Overview

Large Market Opportunity – Acute Pain 8 45M patients receive IV opioids annually to treat acute pain 1 IV opioids have unrivalled analgesic efficacy Top surgeries: Total knee arthroplasty, colectomy, hernia repair, spine fusion, C - section 2 IV NSAIDS / acetaminophen US injectable analgesic hospital market unit volume 1 IV opioids 45% IV Opioids 17% 38% Local anesthetics OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . Opioids are associated with serious, potentially life - threatening adverse reactions. NSAIDs = nonsteroidal anti - inflammatory drugs. 1) IMS MIDAS sales audit 2017; IV NSAIDs and Ofirmev ®. 2) Definitive database, and National Vital Statistics report, CDC 2018.

OLINVYK: Differentiated Profile for Acute Pain 9 OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . New chemical entity Distinct from IV morphine IV opioid efficacy Hard - and soft - tissue surgeries Rapid analgesia 1 - 3 min median onset of pain relief Simplified, predictable dosing No adjustment in renal impaired No active metabolites Data in complex patients Elderly / obese, multiple comorbidities Well - characterized safety / tolerability Studied in over 1,900 individuals

VOLITION Clinical Outcomes Study w/ Cleveland Clinic • Open - label, multi - site study led by experts at Cleveland Clinic and Wake Forest Baptist Health • N = 203 adults undergoing major non - cardiac surgery treated with IV OLINVYK • Initial topline data reported 1Q 23 Further characterizes respiratory, GI and cognitive outcomes Respiratory Outcomes GI Tolerability Cognitive Function Assessment via continuous respiratory monitoring (data expected 3Q 23) 52.2% complete GI response 1 defined as no vomiting / no antiemetic use through study period 1 In pooled Phase 3 data for OLINVYK, GI complete response rate was 46.2% (0.35mg) and 39.7% (0.5mg) 90%+ alert / calm at all observation points 2 <4% symptoms of delirium 3 2 Richmond Agitation - Sedation Scale 3 3D - CAM screening tool Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . As with all opioids, serious, life - threatening, or fatal respiratory depression may occur in patients treated with OLINVYK Sedation is an established risk of opioids including OLINVYK CONFIDENTIAL

ARTEMIS – EMR Clinical Outcomes Study • 201 OLINVYK - treated patients at Cleveland Clinic and Wake Forest Baptist Health VOLITION sites • 982 matched patients undergoing similar surgical procedures, treated with other IV opioids, at same sites during VOLITION study - Based on 8 demographic/clinical characteristics (age, sex, type/duration of surgery, overall surgical/medical morbidity, insu ran ce) 11 OLINVYK electronic medical records (EMR) study at VOLITION sites Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . EMR analysis does not provide definitive data of group differences as seen in a prospectively randomized study Matched Patients Treated w/ other IV Opioids (N=982) OLINVYK - Treated VOLITION Patients (N=201) Cost per Admission (avg) $45.9k $37.1k P<0.0001 Hospital Length of Stay (avg) 7.1 days 5.7 days P<0.0001 $8.8k reduction 1.4 day reduction

OLINVYK: Ease of Dosing and Administration • Bolus Dosing: 1 mg and 2 mg vials (single dose) • PCA Dosing: 30 mg vial (single patient use) • OLINVYK 1 mg ≈ morphine 5 mg 1 27 mg cumulative daily dose limit Do not administer single doses greater than 3 mg 12 3 vials allow for flexible and tailored IV dosing No refrigeration / reconstitution $17.50 $25.75 $110.00 WAC: 1 mg / 1mL 30 mg / 30 mL 2 mg / 2mL ~$100 / day (estimated avg cost across procedures) Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . 1) For an initial dose. PCA = Patient - Controlled Analgesia

OLINVYK vs IV Morphine Health Economic Models 13 Published 1 and available to formulary committees * As stated in the label these data are not an adequate basis for comparison of rates between OLINVYK treatment group and the mo rphine treatment group. The OLINVYK and morphine dosing regimens studied are not considered equipotent. 1) Simpson KN, et al., J Comp Eff Res, 2021 ; 10:1107 - 1119 and Simpson KN, et al. Expert Rev Pharmacoecon Outcomes Res; 2022 2) Oderda , GM, J Pain Palliative Care Pharm, 2019; data based on 5 surgical procedure categories including Cardiothoracic / vascular, Gen eral / Colorectal, Ob / Gyn, Orthopedic, and Urologic. 3) Overdyk FJ, PLoS One, 2016. More conservative inputs were used in the model. 4) Calculated based on total costs of Tx and average total costs of care. Image: flaticon.com. Vomiting Somnolence / sedation O 2 saturation <90% Representative Inputs: >10x Cost savings for hospitals 4 Due to improved patient outcomes HECON model Placebo (N = 162) OLINVYK ≤ 27 mg (N = 316) Morphine (N = 158) Patients with any TEAE (%) 73 86 96 Nausea 35 52 70 Vomiting 10 26 52 Headache 30 26 30 Dizziness 11 18 25 Constipation 9 14 14 Hypoxia 3 12 17 Pruritus 6 9 19 Sedation 5 7 13 Somnolence 4 6 10 Back pain 4 6 6 Hot flush 4 4 8 Pruritus gen. 1 2 10 AE rates * Cost of AEs Drug cost Ph3 trials Gov’t sources / Publications $8k nausea / vomiting 2 $28k critical resp event 3 +7 days hospital stay 3 OLINVYK IV morphine Key Outputs:

OLINVYK: Significant Opportunity in Acute Pain Market 14 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . Source: Definitive Healthcare; American Hospital Association. *Assumes ~$100 / day price for OLINVYK 2032 composition of matter patent expiration does not include potential patent extensions. Specialty Targets Patient & Procedure Risk Initial launch focus ~45 M patients Initial core focus: (9 M ) Expanded areas of focus: (28 M ) • Ambulatory surgical centers • Hospitals Core focus ~15M days of therapy (initial focus) = $1.5B+ market opportunity* • New cognitive function / respiratory / GI data versus IV morphine • Additional HECON data focused on recovery time Expanded areas of focus 2032+ COM Patent

TRV045 S1P Receptor Modulator Novel MOA for Diabetic Neuropathic Pain

S1P 1 Receptor – Novel Target for CNS Indications 1) Sim - Selley et al., Journal of Pharmacology & Experimental Therapeutics, 2018. 2) Sim - Selley et al, Journal of Neurochemistry, 2008. 3) Gol et al., European Journal of Pharmaceutical Sciences, 2017. 4) Leo et al, CNS & Neurological Disorders - Drug Targets, 2017. 5) Choi, et al. PNAS 2011. S1P 1 receptors are highly expressed on key CNS cells involved in neuroinflammation Potential therapeutic role in seizures, epileptogenesis and pain signaling Neuropathic pain • Inhibits pain sensation 1 • Inhibits excitatory neuronal signaling 2 Existing S1PR - targeted drugs, however, are ill - suited for CNS indications due to known: Lymphopenia Pulmonary AEs Cardiac AEs Ophthalmologic AEs Epilepsy • Neuroprotective effects 3 • Modulates BBB permeability, anti - inflammatory effects 4,5 16

TRV045 MOA: Rapid Receptor Recycling b - arrestin2 S1P 1 receptor G GRK Internalization ↑ I K Ach ligand G a i cAMP Ca++ (via IcaL ) Reduces surface receptor, which leads to lymphopenia ( Gilenya , etc ) Receptor R ecycling Maintains surface receptor and avoids lymphopenia, allowing free lymphocyte egress into circulation Receptor Degradation Other S1PR Drugs TRV045 17 Maintained (rather than degraded) S1P receptors on cell surface No lymphopenia reported in prior Phase 1 FIH study Maintained surface receptor, allowing free lymphocyte egress into circulation FIH = First in human Source: Trevena data on file

0 1 2 3 4 5 6 Fingolimod TRV045 No Lymphopenia TRV045 Efficacy in Nonclinical Chronic Pain Models (w/ no Lymphopenia) 1) CIPN mouse model: Paclitaxel 6 mg/kg, i.p. on Days 1, 3, 5, 7. Hyperalgesia measured as % non - response to 0.4 g Von Frey filament vs. baseline, tested 30’ after dosing on Day 13. Lymphocytes measured after 3 days of dosing. Data are mean “ s.e.m. n=5 - 7 mice/group. *p<0.05 or **p<0.01 vs. control peripheral lymphocytes (10 3 cells / m L) 0.03 mg/kg po 3.7 mg/kg sc Vehicle alone No reduction despite 3.7x dosing (vs. above) ** Reversed Pain Response 0 20 40 60 80 100 Fingolimod TRV045 % non - response to pain stimulus 0.03 mg/kg po 1.0 mg/kg sc Paclitaxel - induced hyperalgesia * ** 18 Mouse chemotherapy - induced peripheral neuropathy (CIPN) model Reversed neuropathic pain… …with no lymphopenia Source: Trevena data on file
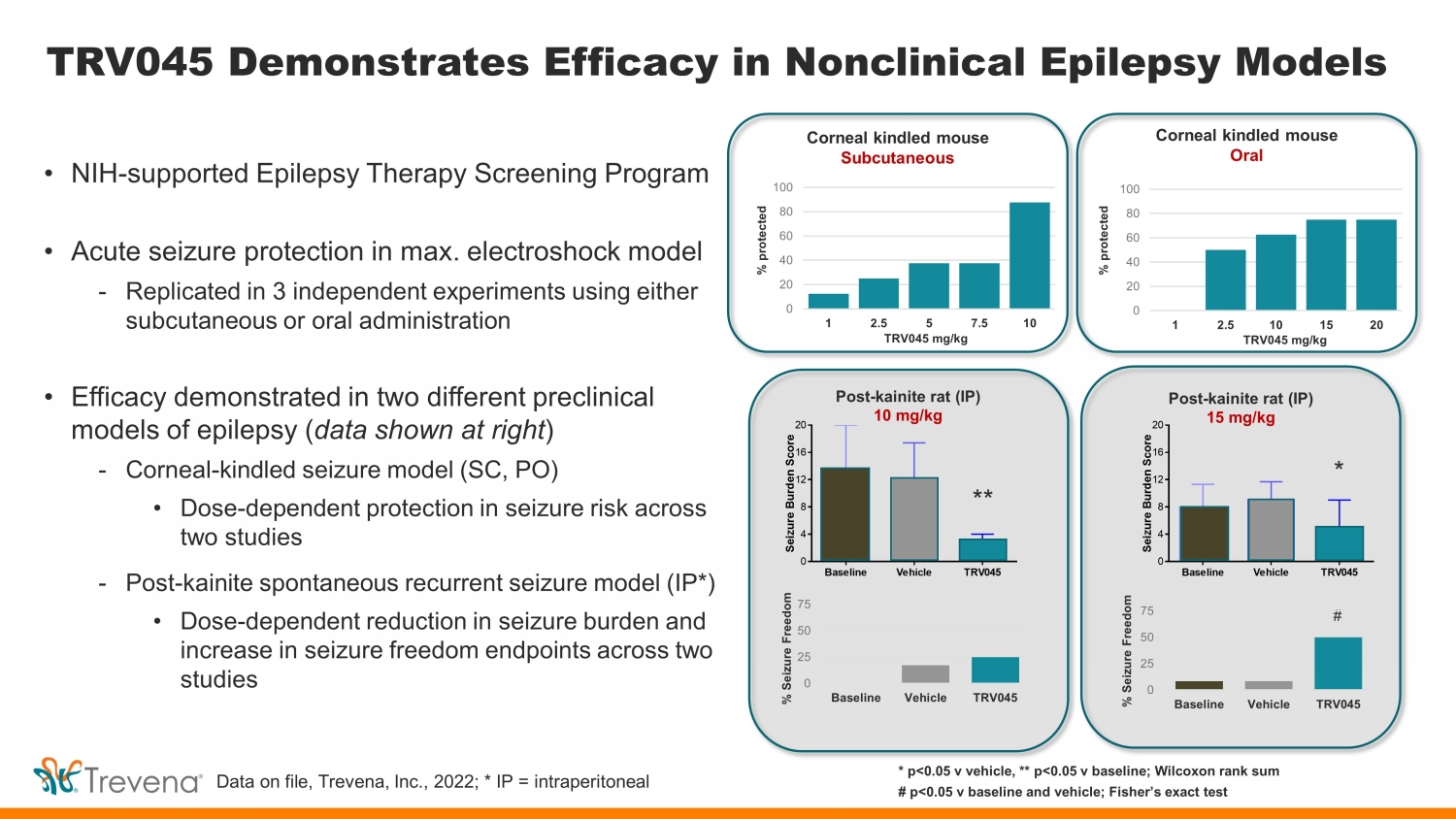
TRV045 Demonstrates Efficacy in Nonclinical Epilepsy Models • NIH - supported Epilepsy Therapy Screening Program • Acute seizure protection in max. electroshock model - Replicated in 3 independent experiments using either subcutaneous or oral administration • Efficacy demonstrated in two different preclinical models of epilepsy ( data shown at right ) - Corneal - kindled seizure model (SC, PO) • Dose - dependent protection in seizure risk across two studies - Post - kainite spontaneous recurrent seizure model (IP*) • Dose - dependent reduction in seizure burden and increase in seizure freedom endpoints across two studies Baseline Vehicle TRV045 0 4 8 12 16 20 S e i z u r e B u r d e n S c o r e * * p<0.05 v vehicle, ** p<0.05 v baseline; Wilcoxon rank sum # p<0.05 v baseline and vehicle; Fisher’s exact test Corneal kindled mouse Subcutaneous Corneal kindled mouse Oral Post - kainite rat (IP) 10 mg/kg Post - kainite rat (IP) 15 mg/kg 0 20 40 60 80 100 1 2.5 5 7.5 10 0 20 40 60 80 100 1 2.5 10 15 20 % protected % protected TRV045 mg/kg TRV045 mg/kg Data on file, Trevena, Inc., 2022; * IP = intraperitoneal ** * # 0 25 50 75 Baseline Vehicle TRV045 % Seizure Freedom 0 25 50 75 Baseline Vehicle TRV045 % Seizure Freedom

TRV045 Phase 1 Study – Safety / Tolerability / PK Randomized, double - blinded, placebo - controlled study 3 - parts: single dose (n=53), food effect (n=27), multiple dose (n=9) 20 • Favorable tolerability profile with no SAEs Well Tolerated Target Exposure Attractive PK Profile • Calculated free plasma concentrations exceeded targeted efficacy range 1 • Half - life consistent with anticipated once - daily dosing Highly Differentiated • No lymphopenia and no reported cardiac / pulmonary / ophthalmologic AEs (AEs commonly associated with currently marketed S1P - targeted compounds) 1 Based on nonclinical measures of in vitro and in vivo PD

Studies were conducted outside the United States and not under the IND for TRV045 POC Studies: Target Engagement / TMS 21 Results confirm activity of central action and support advancement for neuropathic pain and other CNS indications Target Engagem ent Study Randomized, double - blind, placebo - controlled, 4x cross - over (n=25 subjects) Placebo or TRV045 (50 / 150 / 300mg) PainCart ® endpoints TMS Study Randomized, double - blind, placebo - controlled, multiple dose, 2x cross - over (n=25 subjects) Placebo or TRV045 (250mg / four days) EEG / EMG endpoints

TE Study: Significantly Reduced Mechanical Allodynia 22 1% capsaicin - treated dominant volar forearm – Von Frey filament allodynic area (CFB, mm 2 ) Change from Baseline (mm 2) -1200 -1000 -800 -600 -400 -200 0 200 400 600 Baseline Hr 1 Hr 2 Hr 4 Hr 6 Hr 8 Hr 10 Total Allodynic Area Placebo 50mg 150mg 300mg -1200 -1000 -800 -600 -400 -200 0 200 400 600 Baseline Hr 1 Hr 2 Hr 4 Hr 6 Hr 8 Hr 10 Secondary Allodynic Area Placebo 50mg 150mg 300mg 300mg TRV045 v Placebo; P=0.0023 150mg TRV045 v Placebo; P=0.0022 300mg TRV045 v Placebo; P=0.0001 150mg TRV045 v Placebo; P=0.0002 Source: Trevena data on file
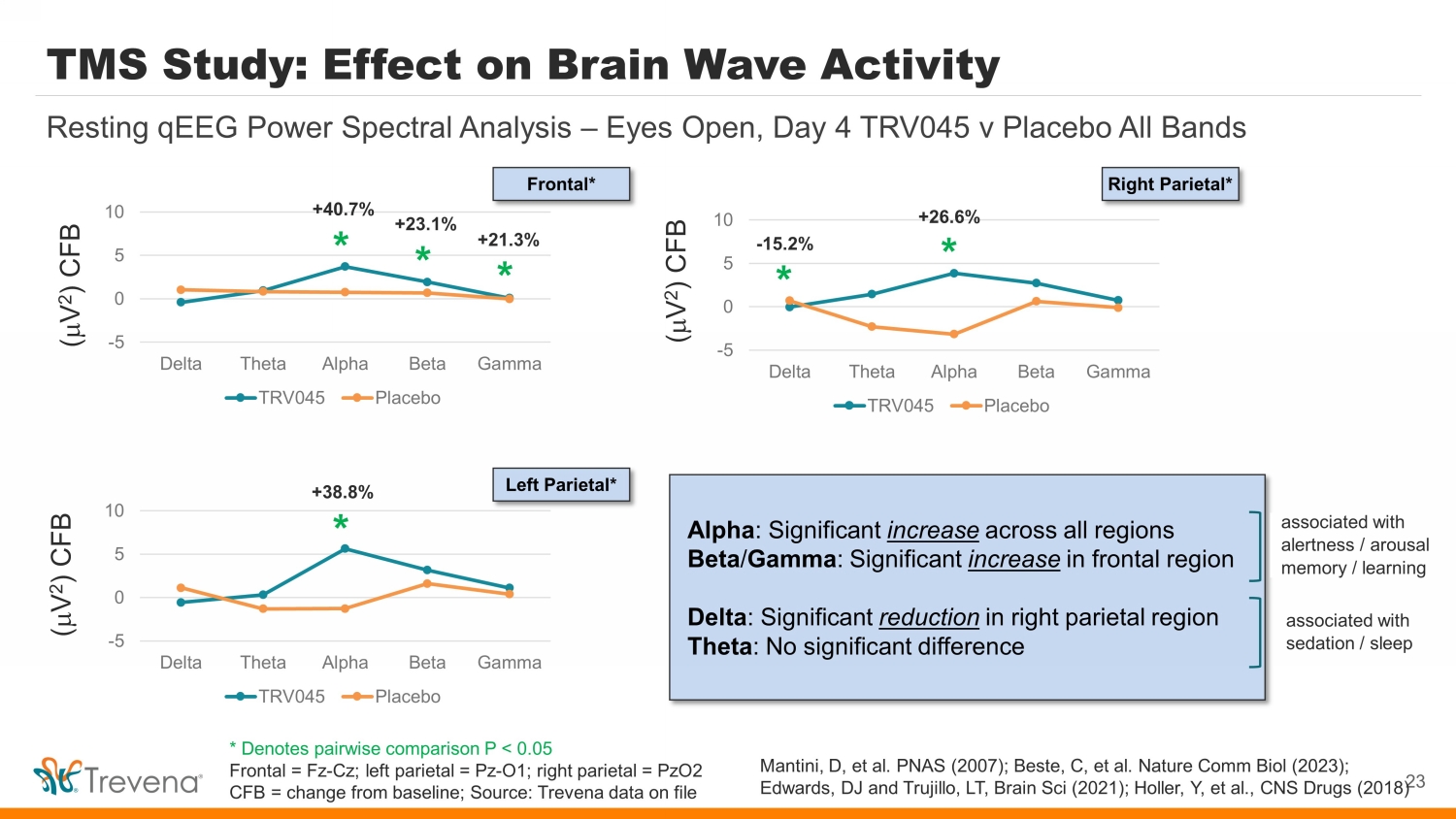
TMS Study: Effect on Brain Wave Activity -5 0 5 10 Delta Theta Alpha Beta Gamma TRV045 Placebo 23 Resting qEEG Power Spectral Analysis – Eyes Open, Day 4 TRV045 v Placebo All Bands -5 0 5 10 Delta Theta Alpha Beta Gamma TRV045 Placebo -5 0 5 10 Delta Theta Alpha Beta Gamma TRV045 Placebo * * * * * * +21.3% - 15.2% +23.1% +40.7% +38.8% +26.6% ( m V 2 ) CFB ( m V 2 ) CFB ( m V 2 ) CFB Frontal* Left Parietal* Right Parietal* Alpha : Significant increase across all regions Beta / Gamma : Significant increase in frontal region Delta : Significant reduction in right parietal region Theta : No significant difference associated with alertness / arousal memory / learning associated with sedation / s leep Mantini , D, et al. PNAS (2007); Beste , C, et al. Nature Comm Biol (2023); Edwards, DJ and Trujillo, LT, Brain Sci (2021); Holler, Y, et al., CNS Drugs (2018) * Denotes pairwise comparison P < 0.05 Frontal = Fz - Cz ; left parietal = Pz - O1; right parietal = PzO2 CFB = change from baseline; Source: Trevena data on file

TMS Study: Effect on Cortical Excitability vs AEDs* Mean change from baseline in MEP on Day 1 with TRV045 comparable in magnitude to MEP reductions seen with known AEDs, including levetiracetam, valproic acid, and lorazepam, performed in the same laboratory 24 Mean change from baseline in motor - evoked potential (MEP) measured by peak - to - peak amplitude Ruijs , TQ, et al. BJCP (2022) 88:2926 - 2937 Estimated difference vs placebo: • Levetiracetam: - 378.4 m V, 95% CI - 644.3 to - 112.5; P<0.01 • Valproic acid: - 268.8 m V, 95% CI - 532.9 to - 4.6; P=0.047 • Lorazepam: - 330.7.4 m V, 95% CI - 595.6 to - 65.8; P=0.02 782.0 840.1 859.0 605.4 0 100 200 300 400 500 600 700 800 900 1000 Placebo Day 1 TRV045 Day 1 Mean Peak Amplitude ( m V) Pre - dose 4h post - dose Est. difference TRV045 v placebo (not stat. sig.) • - 304.14 m V, 95% CI - 688.19 to 79.919 (P=0.1182) * AEDs = Antiepileptic drugs Source: Trevena data on file

Overall TRV045 POC Study Conclusions • Target Engagement. Demonstrated CNS penetration and target engagement • Neuropathic Pain. Statistically significant, dose - dependent effect in validated model of neuropathic pain • EEG Spectral Power. Statistically significant increases in brain waves (alpha, beta, gamma) associated with arousal , alertness , cognitive processing , learning and memory Statistically significant decrease in delta brain waves, and no significant change in theta brain waves, which are both associated with sedation / sleep • Cortical Excitability. Promising evidence of early reduction in cortical excitability TRV045 Proof - of - Concept Study Program Taken together, these two POC studies provide strong support and direction for future development of TRV045 Studies were conducted outside the United States and not under the IND for TRV045

TRV734: Maintenance Therapy for Opioid Use Disorder

TRV734: Maintenance Therapy for Opioid Use Disorder 27 Selective agonism at µ receptor: nonclinical evidence of improved tolerability 1) Center for Behavioral Health Statistics and Quality. 2) NIDA data on file. Ongoing collaboration with National Institute on Drug Abuse (NIDA) >2.5M people in U.S. suffer from opioid use disorder 1 NIDA study demonstrated reduced drug - seeking behavior in animal model of relapse 2 NIDA - funded proof - of - concept patient study initiated • Randomized, double - blind, placebo - and positive - controlled study • N = ~50 opioid - dependent patients undergoing stable methadone maintenance therapy • Primary endpoint: s uppression of withdrawal symptoms as measured by the Subjective Opioid Withdrawal Scale • Secondary outcomes: assessments of safety, tolerability, and neurocognitive changes

Trevena: Innovative CNS Company 28 *OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . PoC = Proof of concept, NCE = New Chemical Entity; MOA = Mechanism of Action; NIH = National Institutes of Health IV OLINVYK: Differentiated profile TRV045: Selective S1PR modulator Novel CNS pipeline TRV045: Compelling PoC Data Financial position NCE approved for the management of acute pain in adults* Significant cost savings / differentiation shown in ‘real world’ post - approval studies S1PR: Validated target for blockbusters (fingolimod / siponimod / ozanimod / ponesimod ) TRV045: Unique profile (no lymphopenia) for new indications New mechanisms for acute / neuropathic pain, epilepsy, acute migraine, opioid use disorder NCEs targeting significant unmet needs Statistically significant, dose - dependent effect in validated model of neuropathic pain Statistically significant EEG changes and e vidence of early reduction in cortical excitability $28.1M cash / equivalents / marketable securities @ 2Q 23 $15M non - dilutive tranche received 3Q 23 (ex - US royalty based financing)

29 IMPORTANT SAFETY INFORMATION

WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE - THREATENING RESPIRATORY DEPRESSION; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISKS FROM CONCOMITANT USE WITH BENZODIAZEPINES OR OTHER CENTRAL NERVOUS SYSTEM (CNS) DEPRESSANTS Addiction, Abuse, and Misuse OLINVYK exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing OLINVYK, and monitor all patients regularly for the development of behaviors or conditions. Life - Threatening Respiratory Depression Serious, life - threatening, or fatal respiratory depression may occur with use of OLINVYK. Monitor for respiratory depression, especially during initiation of OLINVYK or following a dose increase. Neonatal Opioid Withdrawal Syndrome Prolonged use of OLINVYK during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life - threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. Risk From Concomitant Use With Benzodiazepines or Other CNS Depressants Concomitant use of opioids with benzodiazepines or other CNS depressants, including alcohol, may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing for use in patients for whom alternative treatment options are inadequate; limit dosages and durations to the minimum required; and follow patients for signs and symptoms of respiratory depression and sedation. Limitations of Use Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, reserve OLINVYK for use in patients for whom alternative treatment options [e.g., non - opioid analgesics or opioid combination products]: • Have not been tolerated, or are not expected to be tolerated • Have not provided adequate analgesia, or are not expected to provide adequate analgesia. The cumulative total daily dose should not exceed 27 mg, as total daily doses greater than 27 mg may increase the risk for QTc interval prolongation. CONTRAINDICATIONS OLINVYK is contraindicated in patients with: Significant respiratory depression Acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment Known or suspected gastrointestinal obstruction, including paralytic ileus Known hypersensitivity to oliceridine (e.g., anaphylaxis) WARNINGS AND PRECAUTIONS OLINVYK contains oliceridine, a Schedule II controlled substance, that exposes users to the risks of addiction, abuse, and misuse. Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed OLINVYK. Assess risk, counsel, and monitor all patients receiving opioids. Serious, life - threatening respiratory depression has been reported with the use of opioids, even when used as recommended, especially in patients with chronic pulmonary disease, or in elderly, cachectic and debilitated patients. The risk is greatest during initiation of OLINVYK therapy, following a dose increase, or when used with other drugs that depress respiration. Proper dosing of OLINVYK is essential, especially when converting patients from another opioid product to avoid overdose. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status. Opioids can cause sleep - related breathing disorders including central sleep apnea (CSA) and sleep - related hypoxemia with risk increasing in a dose - dependent fashion. In patients who present with CSA, consider decreasing the dose of opioid using best practices for opioid taper. INDICATIONS AND USAGE OLINVYK is a new chemical entity indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. 30

WARNINGS AND PRECAUTIONS Prolonged use of opioids during pregnancy can result in withdrawal in the neonate that may be life - threatening. Observe newborns for signs of neonatal opioid withdrawal syndrome and manage accordingly. Advise pregnant women using OLINVYK for a prolonged period of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. P r o f ound s e d a tion, re spi r a to r y d e p r e ssion, c om a , a nd d ea th m a y re sult f r om the c on c omit a nt use of OLINVYK with b e n z odi a z e pin e s or oth e r C NS d e p re ss a nts ( e . g ., non - b e n z odi a z e pine s e d a tiv e s/ h y pnoti c s, a n x i o l y ti c s, t ra nquili z er s, mus c le re l a x a nts, g e n e ra l a n e sth e ti c s, a ntip s y c hoti c s, oth e r opioids, or a l c ohol ) . B e ca u s e o f th e se r isks, re s er ve c o n c omit a nt p re s cr ibi n g of th e se d r u g s f o r use in p a ti e nts f or whom a lt er n a tive t rea tm e nt options a r e in a d e qu a t e , prescribe the lowest effective dose, and minimize the duration. OLINVYK was shown to have mild QTc interval prolongation in thorough QT studies where patients were dosed up to 27 mg. Total cumulative daily doses exceeding 27 mg per day were not studied and may increase the risk for QTc interval prolongation. Therefore, the cumulative total daily dose of OLINVYK should not exceed 27 mg. Increased plasma concentrations of OLINVYK may occur in patients with decreased Cytochrome P450 (CYP) 2D6 function or normal metabolizers taking moderate or strong CYP2D6 inhibitors ; also in patients taking a moderate or strong CYP3A4 inhibitor, in patients with decreased CYP2D6 function who are also receiving a moderate or strong CYP3A4 inhibitor, or with discontinuation of a CYP3A4 inducer. These patients may require less frequent dosing and should be closely monitored for respiratory depression and sedation at frequent intervals. Concomitant use of OLINVYK with CYP3A4 inducers or discontinuation of a moderate or strong CYP3A4 inhibitor can lower the expected concentration, which may decrease efficacy, and may require supplemental doses. Cases of adrenal insufficiency have been reported with opioid use (usually greater than one month). Presentation and symptoms may be nonspecific and include nausea, vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure. If confirmed, treat with physiologic replacement doses of corticosteroids and wean patient from the opioid. OLINVYK m a y ca u s e s e v e r e h y po t e ns i o n, i n c l u d i n g or t h o s tatic h y po t e ns i o n a n d s yn c op e in a m b u lat o r y p atie n t s . T h e r e is i n c r ea s ed r i s k in p ati e n ts w ho s e a b ili t y to m a i n ta i n b l oo d pr e ssu r e h as a l r ea d y b een c o m pr o m i s ed b y a r e d u ced b l oo d v o l u m e o r c o n c u rr e n t a d m i n i s t r ati o n o f c e r tain C N S d e pr e ss a n t dru g s ( e . g . , phenothiazines or g e n e r al a n e s t h eti c s ). M o n it o r t h e s e p atie n ts f o r s i g n s o f h y po t e ns i o n. I n p atie n t s w i t h ci r c u lat o r y s h o c k , avoid the use of OLINVYK as it m a y c a us e v a s od ilati o n t h at can f u r t h er r e d u ce ca rd iac o u t p u t a n d b l oo d pr e ssu r e. A v o id t h e us e o f OLINVYK in p atie n ts w i th i m p ai r ed c o ns ci o u s n e s s o r c o m a. OLINVYK should be used with caution in p atie n ts w h o m a y b e s us ce p ti b le to t h e i n t r ac r a n ial e f f ec t s o f C O 2 r et e n ti o n, such as t h o s e with e v i d e n ce o f i n c r ea s ed i n t r ac r a n ial pr e s su r e o r br ain t u m or s , as a reduction in r e s p i r at or y dr i v e a n d t h e r e su lt a n t C O 2 r et e n ti o n can f u r t h er i n c r ea s e i n t r ac r a n i al pr e ssu r e. Mo n it o r su c h p at i e n ts f o r s i g n s o f s e d ati o n a n d r e s p i r at or y d e pr e ss i o n , p a r tic u la r l y w h en i n i t iat i n g t h e r a p y. As with all opioids, OLINVYK m a y ca u s e s p a s m o f t h e s p h i n c ter o f O dd i , and m a y ca us e i n c r ea s es i n s e r u m a my la s e. Mo n it o r p atie n ts w i t h b ilia r y t r act d i s ea s e, i n c l u d i n g a c u te p a n c r eatit i s , f o r w o r s e n i n g s y m p t o ms . T h e r e is i n c r ea s ed r i s k in p ati e n ts w ho s e a b ili t y to m a i n ta i n b l oo d pr e ssu r e h as a l r ea d y b een c o m pr o m i s ed b y a r e d u ced b l oo d v o l u m e o r c o n c u rr e n t a d m i n i s t r ati o n o f c e r tain C N S d e pr e ss a n t dru g s ( e . g . , phenothiazines or g e n e r al a n e s t h eti c s ). M o n it o r t h e s e p atie n ts f o r s i g n s o f h y po t e ns i o n. I n p atie n t s w i t h ci r c u lat o r y s h o c k , avoid the use of OLINVYK as it m a y c a us e v a s od ilati o n t h at can f u r t h er r e d u ce ca rd iac o u t p u t a n d b l oo d pr e ssu r e. A v o id t h e us e o f OLINVYK in p atie n ts w i th i m p ai r ed c o ns ci o u s n e s s o r c o m a. OLINVYK should be used with caution in p atie n ts w h o m a y b e s us ce p ti b le to t h e i n t r ac r a n ial e f f ec t s o f C O 2 r et e n ti o n, such as t h o s e with e v i d e n ce o f i n c r ea s ed i n t r ac r a n ial pr e s su r e o r br ain t u m or s , as a reduction in r e s p i r at or y dr i v e a n d t h e r e su lt a n t C O 2 r et e n ti o n can f u r t h er i n c r ea s e i n t r ac r a n i al pr e ssu r e. Mo n it o r su c h p at i e n ts f o r s i g n s o f s e d ati o n a n d r e s p i r at or y d e pr e ss i o n , p a r tic u la r l y w h en i n i t iat i n g t h e r a p y. As with all opioids, OLINVYK m a y ca u s e s p a s m o f t h e s p h i n c ter o f O dd i , and m a y ca us e i n c r ea s es i n s e r u m a my la s e. Mo n it o r p atie n ts w i t h b ilia r y t r act d i s ea s e, i n c l u d i n g a c u te p a n c r eatit i s , f o r w o r s e n i n g s y m p t o ms . OLINVYK m a y i n c r ea s e t h e f r e q u e n c y o f s ei z u r es i n p atie n t s w i t h s eiz u r e d i s ord e r s a n d may increase t h e r i s k o f s ei z u r es in vulnerable patients . M o n it o r p atie n ts w i th a h i s t o r y o f s ei z u r e d i s ord e r s f o r w or s e n ed s eiz u r e c o n t ro l. Do not abruptly discontinue OLINVYK in a patient physically dependent on opioids. Gradually taper the dosage to avoid a withdrawal syndrome and return of pain. Avoid the use of mixed agonist/antagonist (e.g., pentazocine , nalbuphine , and butorphanol ) or partial agonist (e.g., buprenorphine) analgesics in patients who are receiving OLINVYK, as they may reduce the analgesic effect and/or precipitate withdrawal symptoms. OLINVYK may impair the mental or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Although self - administration of opioids by patient - controlled analgesia (PCA) may allow each patient to individually titrate to an acceptable level of analgesia, PCA administration has resulted in adverse outcomes and episodes of respiratory depression. Health care providers and family members monitoring patients receiving PCA analgesia should be instructed in the need for appropriate monitoring for excessive sedation, respiratory depression, or other adverse effects of opioid medications. ADVERSE REACTIONS Adverse reactions are described in greater detail in the Prescribing Information. The most common (incidence ≥10%) adverse reactions in Phase 3 controlled clinical trials were nausea, vomiting, dizziness, headache, constipation, pruritus, and hypoxia. PLEASE see www.OLNVYK.com for full prescribing information including BOXED warning and important safety information 31
Exhibit 99.2

| INNOVATING FOR PATIENTS
Nasdaq TRVN I September 2023 |

| Forward-Looking Statements
To the extent that statements contained in this presentation are not descriptions of historical facts regarding Trevena, Inc. (the “Company” or “we”), they are forward-looking statements
reflecting management’s current beliefs and expectations. Forward-looking statements are subject to known and unknown risks, uncertainties, and other factors that may cause our or our
industry’s actual results, levels of activity, performance, or achievements to be materially different from those anticipated by such statements. You can identify forward-looking statements by
terminology such as “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “might,” “plan,” “objective,” “predict,” “project,” “suggest,” “target,” “potential,” “will,” “would,” “could,” “should,”
“continue,” “ongoing,” or the negative of these terms or similar expressions. Forward-looking statements contained in this presentation include, but are not limited to, (i) statements regarding
the timing of anticipated clinical trials for our product candidates; (ii) the timing of receipt of clinical data for our product candidates; (iii) our expectations regarding the potential safety, efficacy,
or clinical utility of our product candidates; (iv) the size of patient populations targeted by our product candidates and market adoption of our potential drugs by physicians and patients; (v) the
timing or likelihood of regulatory filings and approvals; and (vi) our cash needs.
Actual results may differ materially from those indicated by such forward-looking statements as a result of various important factors, including: the commercialization of any approved drug
product, the status, timing, costs, results and interpretation of our clinical trials or any future trials of any of our investigational drug candidates; the uncertainties inherent in conducting clinical
trials; expectations for regulatory interactions, submissions and approvals, including our assessment of the discussions with the FDA or other regulatory agencies about any and all of our
programs; uncertainties related to the commercialization of OLINVYK; available funding; uncertainties related to our intellectual property; other matters that could affect the availability or
commercial potential of our therapeutic candidates; and other factors discussed in the Risk Factors set forth in our Annual Report on Form 10-K and Quarterly Reports on Form 10-Q filed
with the Securities and Exchange Commission (SEC) and in other filings we make with the SEC from time to time. In addition, the forward-looking statements included in this presentation
represent our views only as of the date hereof. We anticipate that subsequent events and developments may cause our views to change. However, while we may elect to update these
forward-looking statements at some point in the future, we specifically disclaim any obligation to do so, except as may be required by law.
2 |

| Trevena Overview
3
Focused on Innovative Medicines
For CNS Disorders
Olinvyk IV*
Approved NCE for the
management of acute pain in
adults*
Proven track record of Trevena
internal discovery and
development through approval
S1P Modulator Program
Novel S1P1R modulator with
differentiated MOA (lead
asset: TRV045)
Preliminary data from proof-of-concept studies for
CNS disorders
Innovative CNS Pipeline
Based on Nobel-prize
winning biased ligand
technology
NCEs addressing acute /
neuropathic pain, epilepsy,
acute migraine, OUD1
Detailed in Following Slides
* OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom
alternative treatments are inadequate.
Please see Important Safety Information including BOXED WARNING at the end of presentation.
Full Prescribing Information at www.OLINVYK.com. 1 OUD = opioid use disorder |

| TRV045: Innovative Clinical-Stage S1P1R Modulator
TRV045:
Selective S1PR Modulator
Compelling Clinical
POC Data
Strong MOA
Support
Large Addressable Target
Indications
Novel Family of
S1PR Modulators
S1PR: Validated target for multiple blockbusters (fingolimod / siponimod / ozanimod / ponesimod)
TRV045: Unique profile (S1P1R specific, receptor recycling, no lymphopenia) for new indications
Statistically significant, dose-dependent effect in validated model of neuropathic pain
Statistically significant EEG changes and evidence of early reduction in cortical excitability
Nonclinical models demonstrated positive efficacy outcomes, avoiding known S1PR safety issues
NIH collaboration: Epilepsy Therapy Screening Program & Preclinical Screening Pain Platform
Initial investigation for orphan / non-orphan non-opioid chronic pain and epilepsy
Broad potential application in CNS disorders, autoimmune disease and inflammatory disease
New chemical entity; potent and selective for subtype 1; developed in-house with strong IP
Platform of S1PR backup opportunities for longer term value creation
4 |

| S1P1 Receptor – Novel Target for CNS Indications
1) Sim-Selley et al., Journal of Pharmacology & Experimental Therapeutics, 2018. 2) Sim-Selley et al, Journal of Neurochemistry, 2008. 3) Gol et al., European Journal of
Pharmaceutical Sciences, 2017. 4) Leo et al, CNS & Neurological Disorders - Drug Targets, 2017. 5) Choi, et al. PNAS 2011.
S1P1 receptors are highly expressed on key CNS cells involved in neuroinflammation
Potential therapeutic role in seizures, epileptogenesis and pain signaling
Neuropathic pain
• Inhibits pain sensation1
• Inhibits excitatory neuronal signaling2
Existing S1PR-targeted drugs, however, are ill-suited for CNS indications due to known:
Lymphopenia Pulmonary AEs
Cardiac AEs Ophthalmologic AEs
Epilepsy
• Neuroprotective effects3
• Modulates BBB permeability,
anti-inflammatory effects4,5
5 |

| TRV045 MOA (1): Rapid Receptor Recycling
β-arrestin2
S1P1 receptor
Gβγ GRK
↑I Internalization KAch
ligand
Gαi
↓cAMP
↓ Ca++
(via IcaL)
Reduces surface receptor,
which leads to lymphopenia
(Gilenya, etc)
Receptor Recycling
Maintains surface receptor and
avoids lymphopenia, allowing free
lymphocyte egress into circulation
Receptor Degradation
Other S1PR Drugs TRV045
6
Maintained (rather than degraded) S1P receptors on cell surface
No lymphopenia
reported in prior
Phase 1 FIH study
Maintained surface receptor,
allowing free lymphocyte egress
into circulation
FIH = First in human
Source: Trevena data on file |

| Highly expressed in key
CNS / brain cells
TRV045 MOA (2): S1PR Subtype-1 Selectivity
• S1P acts on 5 distinct subtypes of receptors (S1P1-5)
• TRV045 is potent and selective for S1P subtype-1 receptor
- S1P1R is highly expressed on astrocytes / other glial cells
- May play role in central pain signaling, as well as development and
persistence of seizures
7
Subtype-1 is broadly expressed in the CNS and may avoid effects associated with other subtypes
Highly expressed
in brain glial cells
Broader tissue target expression
Adapted from: Chun, J, et al., Drugs (2021) 81:207–231 |

| 1) P<0.05 v vehicle
2) Full cytokine / chemokine panel studied: (Inflammatory markers) – TNFa, IL-6, IL-1b, IL-17, IL-23, IL-33, CCL1, CCL2, CCL20, CXCL5,
CXCL12, CX3CL1, IFNg, Csf2, Substance P; (Anti-inflammatory markers) – IL-10, IL-4. (Trevena, Inc., data on file)
TRV045 MOA (3): Anti-Inflammatory Effect (nonclinical)
• Main Findings: Net anti-inflammatory action (statistically
significant) on astrocyte cytokine / chemokine release
- Increased all anti-inflammatory markers measured1
- Reduced all inflammatory markers measured1
• Method: Primary mouse astrocytes in monolayer cell
culture, incubated for 24hrs w/ 5 µM TRV045
- 17 cytokines / chemokines2 assessed by ELISA
TRV045-affected cytokines / chemokines
play a role in many CNS disorders
(epilepsy, pain, neuropsych / neurodegen diseases)
Anti-inflammatory actions (cytokines / chemokines) on astrocytes in cell culture
8
-150 -100 -50 0 50 100 150
IL-1b
TNFa
IL-17
CXCL5
IL-4
IL-10
% Change from Vehicle
Anti-markers inflammatory Inflammatory markers |

| TRV045 Proof-of-Concept Study Program – Highlights
• Target Engagement. Demonstrated CNS penetration and target engagement
• Neuropathic Pain. Statistically significant, dose-dependent effect in validated model of neuropathic pain
• EEG Spectral Power. Statistically significant increases in brain waves (alpha, beta, gamma) associated
with arousal, alertness, cognitive processing, learning and memory
Statistically significant decrease in delta brain waves, and no significant change in
theta brain waves, both of which are associated with sedation / sleep
• Cortical Excitability. Directional evidence of early reduction in cortical excitability
Preliminary data*
Not all of the results were statistically significant;
details of the findings are presented on the following slides
Studies were conducted outside the United States and not under the IND for TRV045 |

| TRV045 POC Study Program – Overall Objectives
• Provide evidence of CNS penetration and target engagement via pharmacodynamic effects on validated
experimental study endpoints in humans, using:
- Battery of acute and chronic pain models (characterize ‘analgesic phenotype’ for TRV045)
- EEG and EMG measures of changes in resting state brain electrical activity on and off drug and TMS-stimulated brain
cortical excitability
• Provide PK-PD exposure data to guide future formulation development efforts and dose range selection for
future Phase 2 studies
- Prior phase 1 data demonstrated PK profile consistent with anticipated once-daily dosing
• Provide additional safety and tolerability data to support results of initial Phase 1 FIH study
- No lymphopenia
- No cardiovascular signals of concern
- No evidence of ophthalmologic, pulmonary adverse effects
10
Preliminary data*
* Complete safety and tolerability data expected early 4Q 2023
Studies were conducted outside the United States and not under the IND for TRV045
Source: Trevena data on file |

| Target Engagement (PainCart®) POC Study Design
• Pharmacodynamic Endpoints:
- Mechanical allodynia (Von Frey hair testing on capsaicin-treated skin), pressure pain, heat pain (capsaicin-treated,
UVB-exposed, and unexposed skin), cold pain (CPT), electrical pain (stair, burst conditions), conditioned pain
modulation (electrical pain pre- and post-CPT)
• PK exposure parameters (Cmax, t½)
• Safety and tolerability
11
• Design: Randomized, double-blind, placebo-controlled, single dose, four-way cross-over (N=25 subjects;
8F/17M, mean age 37.6 years, range 18-53)
- Placebo or TRV045 (50/150/300mg)
Studies were conducted outside the United States and not under the IND for TRV045
Source: Trevena data on file |

| TRV045 Significantly Reduced Mechanical Allodynia
12
1% capsaicin-treated dominant volar forearm – Von Frey filament allodynic area (CFB, mm2) Change from Baseline (mm2)
-1200
-1000
-800
-600
-400
-200
0
200
400
600
Baseline Hr 1 Hr 2 Hr 4 Hr 6 Hr 8 Hr 10
Total Allodynic Area
Placebo
50mg
150mg
300mg
-1200
-1000
-800
-600
-400
-200
0
200
400
600
Baseline Hr 1 Hr 2 Hr 4 Hr 6 Hr 8 Hr 10
Secondary Allodynic Area
Placebo
50mg
150mg
300mg
300mg TRV045 v Placebo; P=0.0023
150mg TRV045 v Placebo; P=0.0022
300mg TRV045 v Placebo; P=0.0001
150mg TRV045 v Placebo; P=0.0002
Source: Trevena data on file |
| Source: Trevena data on file
Target Engagement (PainCart®) Study
• Statistically significant, dose-dependent, treatment effect in model of capsaicin-induced mechanical allodynia
provides evidence of the therapeutic potential of TRV045 in neuropathic pain
- Recognized and validated study index of central pain processing (‘central sensitization’)
- Note that effect appeared similar with both 150mg and 300mg dose, potentially guiding future decisions on dose range for
use in Phase 2
• Supportive evidence of analgesic action in select other nociceptive models
- Other endpoints did not show trend / statistically significant results (pressure pain / conditioned pain modulation)
• Overall, strong support for CNS penetrance and engagement of pain signaling pathways in the brain
- PK exposure consistent with parameters observed at comparable doses studied under fed conditions in Phase 1 FIH study
• No SAEs, no drug-related study discontinuations; full safety and tolerability data expected early 4Q 23
13
PainCart observations |

| TMS POC Study Design
• TMS-EEG Pharmacodynamic endpoints:
- Resting qEEG power spectral analysis (eyes open/eyes closed): Alpha, Beta, Delta, Gamma, Theta bands
- TMS-evoked EEG response (single and paired-pulse TMS)
• TMS-EMG Pharmacodynamic endpoints:
- Motor-evoked potential (MEP), resting motor threshold (single pulse TMS), paired-pulse TMS
14
• Design: Randomized, double-blind, placebo-controlled, multiple dose, two-way cross-over (n=25 male
subjects; mean age 31.5 years, range 21-55)
- Placebo or TRV045 (250mg) for 4 days; post-dose assessments performed at 4 hours
Studies were conducted outside the United States and not under the IND for TRV045
TMS = Transcranial magnetic stimulation
Source: Trevena data on file |

| EEG Shifts in Alpha, Beta, Gamma, Delta Power Spectra
-5
0
5
10
Delta Theta Alpha Beta Gamma
TRV045 Placebo
15
Resting qEEG Power Spectral Analysis – Eyes Open, Day 4 TRV045 v Placebo All Bands
-5
0
5
10
Delta Theta Alpha Beta Gamma
TRV045 Placebo
-5
0
5
10
Delta Theta Alpha Beta Gamma
TRV045 Placebo
*
*
*
* *
* +21.3% -15.2%
+23.1%
+40.7%
+38.8%
+26.6%
(µ
V
2) CFB (µ
V
2) CFB
(µ
V
2) CFB
Frontal*
Left Parietal*
Right Parietal*
Alpha: Significant increase across all regions
Beta/Gamma: Significant increase in frontal region
Delta: Significant reduction in right parietal region
Theta: No significant difference
associated with
alertness / arousal
memory / learning
associated with
sedation / sleep
Mantini, D, et al. PNAS (2007); Beste, C, et al. Nature Comm Biol (2023);
Edwards, DJ and Trujillo, LT, Brain Sci (2021); Holler, Y, et al., CNS Drugs (2018)
* Denotes pairwise comparison P < 0.05
Frontal = Fz-Cz; left parietal = Pz-O1; right parietal = PzO2
CFB = change from baseline; Source: Trevena data on file |

| TRV045 Effect on Cortical Excitability vs AEDs*
Mean change from baseline in MEP on Day 1 with TRV045 comparable in magnitude to MEP reductions seen
with known AEDs, including levetiracetam, valproic acid, and lorazepam, performed in the same laboratory
16
Mean change from baseline in motor-evoked potential (MEP) measured by peak-to-peak amplitude
Ruijs, TQ, et al. BJCP (2022) 88:2926-2937
Estimated difference vs placebo:
• Levetiracetam: -378.4 µV, 95% CI -644.3 to -112.5; P<0.01
• Valproic acid: -268.8 µV, 95% CI -532.9 to -4.6; P=0.047
• Lorazepam: -330.7.4 µV, 95% CI -595.6 to -65.8; P=0.02
782.0
840.1 859.0
605.4
0
100
200
300
400
500
600
700
800
900
1000
Placebo Day 1 TRV045 Day 1
Mean Peak Amplitude (
µV)
Pre-dose
4h post-dose
Est. difference TRV045 v placebo (not stat. sig.)
• -304.14 µV, 95% CI -688.19 to 79.919 (P=0.1182)
* AEDs = Antiepileptic drugs
Source: Trevena data on file |

| Overall TRV045 POC Study Conclusions
• Target Engagement. Demonstrated CNS penetration and target engagement
• Neuropathic Pain. Statistically significant, dose-dependent effect in validated model of neuropathic pain
• EEG Spectral Power. Statistically significant increases in brain waves (alpha, beta, gamma) associated
with arousal, alertness, cognitive processing, learning and memory
Statistically significant decrease in delta brain waves, and no significant change in
theta brain waves, which are both associated with sedation / sleep
• Cortical Excitability. Promising evidence of early reduction in cortical excitability
Taken together, these two POC studies provide
strong support and direction for future development of TRV045
Studies were conducted outside the United States and not under the IND for TRV045 |

| TRV045: Broad Potential Applicability
Potential fields for development may include: Seizure treatment (anticonvulsant)
Prevention of seizure (epileptogenesis)
Pain (DPN, CIPN)
Autoimmune (MS, RA, UC, Crohn’s Disease)
Neuropsychiatric / neurodegenerative (MDD, schizophrenia, AD, PD)
Potent and selective S1P1R target engagement
anti-inflammatory and nociceptive effects
No lymphopenia (in FIH study)
potentially limits other S1PR modulators
May avoid AEs associated with approved S1PR drugs
cardiac / pulmonary / ophthalmologic
18
Unique MOA Produces Compelling Profile
potential disease-modifying MOA
DPN: diabetic neuropathic pain; CIPN: chemotherapy-induced peripheral neuropathy; MS: multiple sclerosis; RA: rheumatoid arthritis; MDD:
major depressive disorder; AD: Alzheimer’s disease; PD: Parkinson’s disease |

| TRV045: Innovative Clinical-Stage S1P1R Modulator
TRV045:
Selective S1PR Modulator
Compelling Clinical
POC Data
Strong MOA
Support
Large Addressable Target
Indications
Novel Family of
S1PR Modulators
S1PR: Validated target for multiple blockbusters (fingolimod / siponimod / ozanimod / ponesimod)
TRV045: Unique profile (S1P1R specific, receptor recycling, no lymphopenia) for new indications
Statistically significant, dose-dependent effect in validated model of neuropathic pain
Statistically significant EEG changes and evidence of early reduction in cortical excitability
Nonclinical models demonstrated positive efficacy outcomes, avoiding known S1PR safety issues
NIH collaboration: Epilepsy Therapy Screening Program & Preclinical Screening Pain Platform
Initial investigation for orphan / non-orphan non-opioid chronic pain and epilepsy
Broad potential application in CNS disorders, autoimmune disease and inflammatory disease
New chemical entity; potent and selective for subtype 1; developed in-house with strong IP
Platform of S1PR backup opportunities for longer term value creation
19 |

| TRV045
Prior FIH Phase 1 Study |

| TRV045 Phase 1 Study – Safety / Tolerability / PK
Randomized, double-blinded, placebo-controlled study
3-parts: single dose (n=53), food effect (n=27), multiple dose (n=9)
21
Well Tolerated • Favorable tolerability profile with no SAEs
Target
Exposure
Attractive PK
Profile
• Calculated free plasma concentrations exceeded targeted efficacy range1
• Half-life consistent with anticipated once-daily dosing
Highly
Differentiated
• No lymphopenia and no reported cardiac / pulmonary / ophthalmologic AEs
(AEs commonly associated with currently marketed S1P-targeted compounds)
1 Based on nonclinical measures of in vitro and in vivo PD |

| TRV045
Nonclinical Data - Epilepsy |

| TRV045 demonstrated
dose-dependent protection in seizure risk
in corneal-kindled seizure models
Corneal-kindled Seizure Model
TRV045: Dose Dependent Seizure Protection (nonclinical)
23
Corneal kindled mouse
Subcutaneous
0
20
40
60
80
100
1 2.5 5 7.5 10
% protected
TRV045 mg/kg
Corneal kindled mouse
Oral
0
20
40
60
80
100
1 2.5 10 15 20
% protected
TRV045 mg/kg
Data from NIH-supported Epilepsy Therapy Screening Program |

| B ase line Ve hicle T RV045
0
4
8
1 2
1 6
2 0
Seizure B urden S core
*
15 mg/kg
*
#
0
25
50
75
% Seizure Freedom
Baseline Vehicle TRV045
B ase line Ve hicle T RV045
0
4
8
1 2
1 6
2 0
Seizure B urden S core
*
10 mg/kg
**
0
25
50
75
% Seizure Freedom
Baseline Vehicle TRV045
TRV045 demonstrated a dose-dependent reduction in
seizure burden and increase in seizure freedom
in post-kainate spontaneous recurrent seizure models
Post-kainate Spontaneous Recurrent Seizure Model
TRV045: Improved Seizure Burden / Freedom in
Nonclinical Model
24
* p<0.05 v vehicle, ** p<0.05 v baseline; Wilcoxon rank sum
# p<0.05 v baseline and vehicle; Fisher’s exact test
Data from NIH-supported Epilepsy Therapy Screening Program |

| TRV045 demonstrated
protection from acute seizures
in three replicated experiments
TRV045: Protection from Acute Seizures in
Nonclinical Model
25
Maximal Electroshock Model
0 5 1 0 1 5 2 0 2 5 3 0 3 5
0
2 0
4 0
6 0
8 0
TR V045 m g/kg s.c.
% of rats protected
Maximal electroshock
Subcutaneous
0 1 0 2 0 3 0 4 0 5 0 6 0
0
1 0
2 0
3 0
4 0
TR V045 m g/kg p.o.
% of rats protected
Maximal electroshock
Oral
(data from 2 studies)
Data from NIH-supported Epilepsy Therapy Screening Program |

| TRV045
Nonclinical Data – Non-opioid Pain Indications |

| 0
1
2
3
4
5
6
Fingolimod TRV045
No Lymphopenia
TRV045 Efficacy in Nonclinical Chronic Pain Models (w/ no
Lymphopenia)
1) CIPN mouse model: Paclitaxel 6 mg/kg, i.p. on Days 1, 3, 5, 7. Hyperalgesia measured as % non-response to 0.4 g Von Frey filament vs. baseline, tested 30’ after dosing on Day 13.
Lymphocytes measured after 3 days of dosing. Data are mean ± s.e.m. n=5-7 mice/group. *p<0.05 or **p<0.01 vs. control
peripheral lymphocytes
(103 cells /
µL)
0.03 mg/kg po 3.7 mg/kg sc
Vehicle
alone
No
reduction
despite 3.7x
dosing
(vs. above)
**
Reversed Pain Response
0
20
40
60
80
100
Fingolimod TRV045
% non-response
to pain stimulus
0.03 mg/kg po 1.0 mg/kg sc
Paclitaxel- induced
hyperalgesia
*
**
27
Mouse chemotherapy-induced peripheral neuropathy (CIPN) model
Reversed neuropathic pain…
…with no lymphopenia
Source: Trevena data on file |

| Rat diabetic peripheral neuropathic pain (STZ) model
TRV045: Reversed Hyperalgesia in Nonclinical Model
28
Veh 1 0 3 0 6 0 gabap
0
5
1 0
1 5
2 0
2 5
50% W ithdraw al Threshold (g)
STZ
TR V 045 (m g/kg, p.o.)
Effective on
thermal pain endpoint
Effective on
mechanical pain endpoint
Source: Trevena data on file |

| 29
IMPORTANT SAFETY INFORMATION |

| WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY
DEPRESSION; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISKS FROM
CONCOMITANT USE WITH BENZODIAZEPINES OR OTHER CENTRAL NERVOUS
SYSTEM (CNS) DEPRESSANTS
Addiction, Abuse, and Misuse
OLINVYK exposes patients and other users to the risks of opioid addiction, abuse, and
misuse, which can lead to overdose and death. Assess each patient’s risk before
prescribing OLINVYK, and monitor all patients regularly for the development of
behaviors or conditions.
Life-Threatening Respiratory Depression
Serious, life-threatening, or fatal respiratory depression may occur with use of OLINVYK.
Monitor for respiratory depression, especially during initiation of OLINVYK or following a dose
increase.
Neonatal Opioid Withdrawal Syndrome
Prolonged use of OLINVYK during pregnancy can result in neonatal opioid withdrawal
syndrome, which may be life-threatening if not recognized and treated, and requires
management according to protocols developed by neonatology experts. If opioid use is required
for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid
withdrawal syndrome and ensure that appropriate treatment will be available.
Risk From Concomitant Use With Benzodiazepines or Other CNS Depressants
Concomitant use of opioids with benzodiazepines or other CNS depressants, including alcohol,
may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant
prescribing for use in patients for whom alternative treatment options are inadequate; limit
dosages and durations to the minimum required; and follow patients for signs and symptoms of
respiratory depression and sedation.
Limitations of Use
Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, reserve OLINVYK
for use in patients for whom alternative treatment options [e.g., non-opioid analgesics or opioid combination
products]:
• Have not been tolerated, or are not expected to be tolerated
• Have not provided adequate analgesia, or are not expected to provide adequate analgesia.
The cumulative total daily dose should not exceed 27 mg, as total daily doses greater than 27 mg may increase the
risk for QTc interval prolongation.
CONTRAINDICATIONS
OLINVYK is contraindicated in patients with:
• Significant respiratory depression
• Acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment
• Known or suspected gastrointestinal obstruction, including paralytic ileus
• Known hypersensitivity to oliceridine (e.g., anaphylaxis)
WARNINGS AND PRECAUTIONS
• OLINVYK contains oliceridine, a Schedule II controlled substance, that exposes users to the risks of addiction,
abuse, and misuse. Although the risk of addiction in any individual is unknown, it can occur in patients
appropriately prescribed OLINVYK. Assess risk, counsel, and monitor all patients receiving opioids.
• Serious, life-threatening respiratory depression has been reported with the use of opioids, even when used as
recommended, especially in patients with chronic pulmonary disease, or in elderly, cachectic and debilitated
patients. The risk is greatest during initiation of OLINVYK therapy, following a dose increase, or when used
with other drugs that depress respiration. Proper dosing of OLINVYK is essential, especially when converting
patients from another opioid product to avoid overdose. Management of respiratory depression may include
close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical
status.
• Opioids can cause sleep-related breathing disorders including central sleep apnea (CSA) and sleep-related
hypoxemia with risk increasing in a dose-dependent fashion. In patients who present with CSA, consider
decreasing the dose of opioid using best practices for opioid taper.
INDICATIONS AND USAGE
OLINVYK is a new chemical entity indicated in adults for the management of acute pain severe enough to
require an intravenous opioid analgesic and for whom alternative treatments are inadequate.
30 |
| WARNINGS AND PRECAUTIONS
• Prolonged use of opioids during pregnancy can result in withdrawal in the neonate that may be
life-threatening. Observe newborns for signs of neonatal opioid withdrawal syndrome and manage
accordingly. Advise pregnant women using OLINVYK for a prolonged period of the risk of neonatal
opioid withdrawal syndrome and ensure that appropriate treatment will be available.
• Profound sedation, respiratory depression, coma, and death may result from the concomitant use of
OLINVYK with benzodiazepines or other CNS depressants (e.g., non-benzodiazepine sedatives/hypnotics,
anxiolytics, tranquilizers, muscle relaxants, general anesthetics, antipsychotics, other opioids, or alcohol).
Because of these risks, reserve concomitant prescribing of these drugs for use in patients for whom
alternative treatment options are inadequate, prescribe the lowest effective dose, and minimize the duration.
• OLINVYK was shown to have mild QTc interval prolongation in thorough QT studies where patients were
dosed up to 27 mg. Total cumulative daily doses exceeding 27 mg per day were not studied and may
increase the risk for QTc interval prolongation. Therefore, the cumulative total daily dose of OLINVYK
should not exceed 27 mg.
• Increased plasma concentrations of OLINVYK may occur in patients with decreased Cytochrome P450
(CYP) 2D6 function or normal metabolizers taking moderate or strong CYP2D6 inhibitors; also in patients
taking a moderate or strong CYP3A4 inhibitor, in patients with decreased CYP2D6 function who are also
receiving a moderate or strong CYP3A4 inhibitor, or with discontinuation of a CYP3A4 inducer. These
patients may require less frequent dosing and should be closely monitored for respiratory depression and
sedation at frequent intervals. Concomitant use of OLINVYK with CYP3A4 inducers or discontinuation of
a moderate or strong CYP3A4 inhibitor can lower the expected concentration, which may decrease
efficacy, and may require supplemental doses.
• Cases of adrenal insufficiency have been reported with opioid use (usually greater than one month).
Presentation and symptoms may be nonspecific and include nausea, vomiting, anorexia, fatigue, weakness,
dizziness, and low blood pressure. If confirmed, treat with physiologic replacement doses of corticosteroids
and wean patient from the opioid.
• OLINVYK may cause severe hypotension, including orthostatic hypotension and syncope in ambulatory
patients.
• There is increased risk in patients whose ability to maintain blood pressure has already been compromised
by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g.,
phenothiazines or general anesthetics). Monitor these patients for signs of hypotension. In patients with
circulatory shock, avoid the use of OLINVYK as it may cause vasodilation that can further reduce cardiac
output and blood pressure.
• Avoid the use of OLINVYK in patients with impaired consciousness or coma. OLINVYK should be used
with caution in patients who may be susceptible to the intracranial effects of CO2 retention, such as those
with evidence of increased intracranial pressure or brain tumors, as a reduction in respiratory drive and the
resultant CO2 retention can further increase intracranial pressure. Monitor such patients for signs of
sedation and respiratory depression, particularly when initiating therapy.
• As with all opioids, OLINVYK may cause spasm of the sphincter of Oddi, and may cause increases in
serum amylase. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening
symptoms.
• There is increased risk in patients whose ability to maintain blood pressure has already been compromised
by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g.,
phenothiazines or general anesthetics). Monitor these patients for signs of hypotension. In patients with
circulatory shock, avoid the use of OLINVYK as it may cause vasodilation that can further reduce cardiac
output and blood pressure.
• Avoid the use of OLINVYK in patients with impaired consciousness or coma. OLINVYK should be used
with caution in patients who may be susceptible to the intracranial effects of CO2 retention, such as those
with evidence of increased intracranial pressure or brain tumors, as a reduction in respiratory drive and the
resultant CO2 retention can further increase intracranial pressure. Monitor such patients for signs of
sedation and respiratory depression, particularly when initiating therapy.
• As with all opioids, OLINVYK may cause spasm of the sphincter of Oddi, and may cause increases in
serum amylase. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening
symptoms.
• OLINVYK may increase the frequency of seizures in patients with seizure disorders and may increase the
risk of seizures in vulnerable patients. Monitor patients with a history of seizure disorders for worsened
seizure control.
• Do not abruptly discontinue OLINVYK in a patient physically dependent on opioids. Gradually taper the
dosage to avoid a withdrawal syndrome and return of pain. Avoid the use of mixed agonist/antagonist (e.g.,
pentazocine, nalbuphine, and butorphanol) or partial agonist (e.g., buprenorphine) analgesics in patients
who are receiving OLINVYK, as they may reduce the analgesic effect and/or precipitate withdrawal
symptoms.
• OLINVYK may impair the mental or physical abilities needed to perform potentially hazardous activities
such as driving a car or operating machinery.
• Although self-administration of opioids by patient-controlled analgesia (PCA) may allow each patient to
individually titrate to an acceptable level of analgesia, PCA administration has resulted in adverse
outcomes and episodes of respiratory depression. Health care providers and family members monitoring
patients receiving PCA analgesia should be instructed in the need for appropriate monitoring for excessive
sedation, respiratory depression, or other adverse effects of opioid medications.
ADVERSE REACTIONS
Adverse reactions are described in greater detail in the Prescribing Information.
The most common (incidence ≥10%) adverse reactions in Phase 3 controlled clinical trials were nausea,
vomiting, dizziness, headache, constipation, pruritus, and hypoxia.
PLEASE see www.OLNVYK.com for full prescribing information including BOXED warning and important safety
information
31 |
Exhibit 99.3
Trevena
Announces Preliminary TRV045 Data from Two Proof-of-Concept Studies Evaluating S1PR Mechanism of Action and CNS Target Engagement
TRV045 Demonstrated
Statistically Significant Analgesic Effect in Capsaicin-induced Model of Neuropathic Pain in Target Engagement POC Study
TMS POC Study
Provided Statistically Significant Evidence of CNS Activity of TRV045 on Day 4 as Measured by EEG Power Spectral Analysis
No SAEs and No
Study Drug-Related Discontinuations were reported; Full Safety and Tolerability Data Expected in early 4Q 2023
Company to Hold
Conference Call on Wednesday, September 6 at 8 a.m. Eastern
CHESTERBROOK, Pa., September 6, 2023
(GLOBE NEWSWIRE) –Trevena, Inc. (Nasdaq: TRVN), a biopharmaceutical company focused on the development and commercialization of
novel medicines for patients with central nervous system (CNS) disorders, today announced preliminary topline data from two Phase 1 proof-of-concept
studies of TRV045, a novel sphingosine-1-phosphate receptor modulator selective for the S1P receptor subtype 1.
“We’re very excited about
the progress we’ve made with TRV045 and I’m pleased that both proof-of-concept studies demonstrated CNS target engagement.
This dataset marks another significant milestone for Trevena and our ongoing commitment to focus on innovative new therapies,”
said Carrie Bourdow, President and CEO of Trevena. “As a novel, non-opioid therapy, we believe TRV045 has the potential to make
a meaningful difference in the lives of patients and we look forward to advancing TRV045, on our own or with a strategic partner, for
potential treatment of neuropathic pain and other CNS disorders.”
Data from both studies demonstrated
CNS penetration and target engagement, as well as plasma exposures in the anticipated active dose range, supporting the therapeutic potential
of TRV045. In a capsaicin-induced neuropathic pain model, a validated model of neuropathic pain, TRV045 showed a statistically significant,
dose-dependent treatment effect. In the transcranial magnetic stimulation (TMS) proof-of-concept study, TRV045 demonstrated statistically
significant changes in the power spectral density in several bands.
“These preliminary studies strongly
suggest to me that this compound has an impact on the central processing of pain, and is potentially working by reducing neural hyperexcitability,”
said Daniel Clauw, MD, Professor of Anesthesiology, Medicine and Psychiatry at the University of Michigan.” There is a clear need
for innovative new medications for the treatment of chronic pain. TRV045’s novel mechanism of action, accompanied by the early
data suggesting it is well tolerated, make this an exciting new potential therapeutic approach.”
Target Engagement (PainCart®)
POC Study
The Target Engagement POC study was
a randomized, double-blind, placebo-controlled, single dose four-way cross-over study (n=25 subjects) designed to evaluate evidence of
target engagement for TRV045, using a select battery of pharmacodynamic outcomes. The study used the validated PainCart® set of analgesic
tests to evaluate potential central and peripheral nervous system effects and to provide insight into the potential anti-inflammatory
actions of TRV045. Each subject received three different single doses of TRV045 (50mg, 150mg and 300mg) and placebo on four separate
visits across the study duration. Plasma exposures of TRV045 in this study were comparable to levels seen in the previously reported
Phase 1, FIH study and reached the anticipated targeted active dose range.
TRV045 demonstrated a statistically
significant, dose-dependent reduction in mechanical allodynia following topical capsaicin application at 150mg and 300mg v. placebo.
Allodynia was assessed by cutaneous pain sensation upon mechanical stimulation with Von Frey hair filaments, a validated model of neuropathic
pain. The difference was measured for each dose of TRV045 compared to placebo as the change from baseline in both the secondary area
of allodynic sensation and the total area of allodynia across 10 hours following the dose of study medication. The change from baseline
in painful surface area at the final 10 hour timepoint is shown below, along with the associated P-values for each treatment difference
across the entire 10 hour period of observation. Differences were evident for both the 150mg and 300mg doses beginning at hour 2 and
continuing through the entire period of study observation at hour 10.
| Outcome |
Treatment |
Change from
Baseline in Painful
Surface Area at
Final 10 Hour
Timepoint (mm2)* |
P-Value
for Overall
Treatment
Difference v
Placebo |
| Total
Allodynic Area (mm2) |
Placebo |
-67.19 |
|
|
| TRV045
50mg |
-211.61 |
|
0.1844 |
| TRV045
150mg |
-389.45 |
|
0.0002 |
| TRV045
300mg |
-731.78 |
|
0.0001 |
| |
|
|
|
|
| Secondary
Allodynic Area (mm2) |
Placebo |
-15.79 |
|
|
| TRV045
50mg |
-54.98 |
|
0.5313 |
| TRV045
150mg |
-186.14 |
|
0.0022 |
| TRV045
300mg |
-393.05 |
|
0.0023 |
* Least squares (LS) mean change from
baseline
TRV045 further demonstrated a dose-dependent
trend in change from baseline in the cold pressor test, and also demonstrated trends in reduction to heat pain detection threshold on
both unexposed and capsaicin-treated forearm skin, on heat pain detection threshold on unexposed skin on the upper back, and pain tolerance
in the electrical burst stimulation test, though these endpoints did not achieve statistical significance. TRV045 did not show a statistically
significant difference or trend compared to placebo in other pain modalities.
TMS POC Study
The TMS POC study was a randomized,
double-blind, placebo-controlled, multiple dose, two-way cross-over study (n=25 subjects) designed to evaluate the pharmacodynamic effects
of TRV045 (250mg) on cortical excitability in healthy male adults, using both EEG and EMG to measure the impact of TRV045 on the electrical
excitation of the brain. The goal of the study was to provide further insight into TRV045 CNS target engagement and mechanism of action
for the potential treatment of epilepsy and other CNS disorders. Each subject received one of two treatment sequences in random order:
TRV045 at a dose of 250mg, followed by placebo; or placebo followed by 250mg of TRV045, each treatment sequence given once daily for
four consecutive days. Plasma exposures of TRV045 in this study were comparable to levels seen in the previously reported Phase 1, FIH
study and reached the anticipated targeted active dose range.
Among the EEG-related endpoints measured
in the study, resting state EEG obtained before and after administration of TRV045, demonstrated statistically significant increases
in the power spectral density on day 4 in several of the middle to higher frequency bands including alpha, beta and gamma waves. The
changes in alpha waves are generally considered to be associated with conscious arousal and alertness, while beta waves are thought to
be associated with GABA-mediated inhibitory cortical neurotransmission, and gamma waves are generally associated with cognitive processing,
learning and memory. Alpha waves demonstrated this statistically significant increase in power in the frontal region (P=0.0164), as well
as both left parietal (P=0.0047), and right parietal (P=0.0418) regions. This statistically significant increase in power was observed
in the frontal region for beta waves (P=0.0235) and gamma waves (P=0.0343).
With respect to slow brain waves, which
are generally associated with sedation or sleep, TRV045 showed a statistically significant decrease in the delta brain waves on day 4
in the right parietal region (P=0.0432), and no significant difference in theta brain waves at any of the three observed regions.
Among the EMG-related endpoints measured
in the study, TRV045 demonstrated evidence of reduction in cortical excitability, as measured by change in peak motor-evoked potential
(MEP) amplitude, on Day 1 comparable in magnitude to the reduction in cortical excitability reported in similar test conditions in the
same laboratory for approved anti-epileptic drugs, though this result did not achieve statistical significance. There was no difference
in mean peak MEP amplitude on Day 4, and no difference in resting motor threshold (RMT) on Day 1 or Day 4 or other EMG-related endpoints.
There were no serious adverse events
reported, and no drug-related discontinuations from either study. Full safety and tolerability data for these studies are not yet available.
This data is expected in early 4Q 2023. In the previously reported Phase 1 study of TRV045, the only adverse event assessed by study
investigators as probably or definitely related to drug was headache in four subjects across all three parts of the study (n=53, n=27,
n=9).
Subjects in both studies were enrolled
outside of the United States, and the studies were not conducted under the Investigational New Drug Application for TRV045.
Conference Call and Webcast Information
The Company will host a conference call
and webcast with the investment community on September 6, 2023 at 8:00 a.m. Eastern Time featuring remarks by Carrie Bourdow, President
and Chief Executive Officer, Mark Demitrack, M.D., Senior Vice President and Chief Medical Officer, and Barry Shin, Chief Financial Officer.
| Title: |
Trevena Business Update
Conference Call & Webcast |
| |
|
| Date: |
Wednesday, September 6, 2023 |
| |
|
| Time: |
8:00 a.m. ET |
| |
|
| Conference Call Details: |
Toll-Free:1-844-825-9789
International:1-412-317-5180
Conference ID: 10178141 |
The conference call will be webcast live from
the Company’s website and will be available via the following links:
| Webcast: |
https://viavid.webcasts.com/starthere.jsp?ei=1610714&tp_key=d4c27074df
https://www.trevena.com/investors/events-presentations/ir-calendar |
The webcast should be accessed 15 minutes prior to the conference
call start time. A replay of the webcast will be available following the conclusion of the live broadcast and will be accessible on the
Company’s website.
About TRV045
TRV045 is a novel, selective sphingosine-1-phosphate
subtype 1 (S1P1) receptor modulator being developed as a potential treatment for acute and chronic neuropathic pain secondary
to diabetic peripheral neuropathy. Through a collaboration with the National Institutes of Health, Trevena is also exploring TRV045 as
a potential treatment for epilepsy.
S1P receptors are located throughout the
body, including the central nervous system, where they are believed to play a role in modulating neurotransmission and membrane excitability.
Trevena's discovery efforts have identified
a family of compounds that are highly selective for the S1P1 receptor. TRV045 reversed thermal hyperalgesia, a measure
of neuropathic pain, in nonclinical models of diabetic peripheral neuropathy and chemotherapy-induced peripheral neuropathy. TRV045 was
not associated with lymphopenia and produced no changes in blood pressure, heart rate, or respiratory function at or above pharmacologically
active doses in nonclinical studies. TRV045 is an investigational product and is not yet approved by the FDA.
About Epilepsy
Epilepsy, one of the most common neurological diseases in the world,
is a chronic disorder characterized by recurrent seizures. Epilepsy is defined as having two or more unprovoked seizures separated by
at least 24 hours or after one seizure with a high risk of more.
A seizure is a sudden surge of electrical activity in the brain caused
by complex chemical changes that occur in nerve cells. Usually, there is a balance of cells that either encourage or stop other brain
cells from sending messages. A seizure occurs when there may be too much or too little electrical activity in the brain causing an imbalance.
Seizures are a symptom of many different disorders that can affect the brain. Nearly 50 million people suffer from epilepsy worldwide,
including 3 million adults and 470,000 children in the U.S. 150,000 new cases of epilepsy are reported in the United States each year.
According to the CDC, 56% of adults living with diagnosed epilepsy continue to have seizures.
About Diabetic Neuropathic Pain
Diabetic neuropathy is a common complication of both type 1 and type
2 diabetes, with pain in the extremities being one of the main symptoms. Other symptoms may include numbness, tingling, allodynia and
hyperalgesia. Diabetic neuropathic pain is usually characterized as moderate to severe in nature and can substantially affect patients’
quality of life as well as their social and psychological well-being.
Approximately 25% of people with diabetes are affected by DNP, equaling
over 5 million people in the U.S. During their lifetime, approximately 50% to 70% of diabetic patients may experience symptoms of
DNP.
About Trevena
Trevena, Inc. is a biopharmaceutical company
focused on the development and commercialization of innovative medicines for patients with CNS disorders. The Company has one approved
product in the United States, OLINVYK® (oliceridine) injection, indicated in adults for the management of acute pain
severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. The Company’s novel
pipeline is based on Nobel Prize winning research and includes three differentiated investigational drug candidates: TRV045 for diabetic
neuropathic pain and epilepsy, TRV250 for the acute treatment of migraine and TRV734 for maintenance treatment of opioid use disorder.
For more information, please visit www.Trevena.com
Forward-Looking Statements
Any statements in this press release about future
expectations, plans and prospects for the Company, including statements about the Company’s strategy, future operations, clinical
development and trials of its therapeutic candidates, plans for potential future product candidates and other statements containing the
words “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,”
“plan,” “predict,” “project,” “suggest,” “target,” “potential,”
“will,” “would,” “could,” “should,” “continue,” and similar expressions,
constitute forward-looking statements within the meaning of The Private Securities Litigation Reform Act of 1995. Actual results may
differ materially from those indicated by such forward-looking statements as a result of various important factors, including: the status,
timing, costs, results and interpretation of the Company’s clinical trials or any future trials of any of the Company’s investigational
drug candidates; the uncertainties inherent in conducting clinical trials; expectations for regulatory interactions, submissions and
approvals, including the Company’s assessment of discussions with FDA; available funding; uncertainties related to the Company’s
intellectual property; other matters that could affect the availability or commercial potential of the Company’s therapeutic candidates
and approved product; and other factors discussed in the Risk Factors set forth in the Company’s Annual Report on Form 10-K and
Quarterly Reports on Form 10-Q filed with the Securities and Exchange Commission (SEC) and in other filings the Company makes with the
SEC from time to time. In addition, the forward-looking statements included in this press release represent the Company’s views
only as of the date hereof. The Company anticipates that subsequent events and developments may cause the Company’s views to change.
However, while the Company may elect to update these forward-looking statements at some point in the future, it specifically disclaims
any obligation to do so, except as may be required by law.
For more information, please contact:
Investor Contact:
Dan Ferry
Managing Director
LifeSci Advisors, LLC
daniel@lifesciadvisors.com
(617) 430-7576
Company Contact:
Bob Yoder
SVP and Chief Business Officer
Trevena, Inc.
(610) 354-8840
Exhibit 99.4
Trevena Announces Receipt of $15 Million Non-Dilutive
Tranche and
Provides General Business Update
$15 million tranche from ex-US royalty-based
financing, triggered by first commercial sale of OLINVYK by Jiangsu Nhwa, Trevena’s partner in China
New OLINVYK respiratory data from VOLITION
~200 patient real-world outcomes study, using continuous respiratory monitoring, expected 3Q 2023
Three OLINVYK abstracts accepted for presentation
at upcoming American Society of Anesthesiologists Meeting in 4Q 2023
Company to participate in upcoming HC Wainwright
conference (September 11-13)
Company to Hold Conference Call on Wednesday,
September 6 at 8 a.m. Eastern Time to discuss TRV045 Proof-of-Concept Data
CHESTERBROOK, Pa., September 6, 2023 (GLOBE
NEWSWIRE) – Trevena, Inc. (Nasdaq: TRVN), a biopharmaceutical company focused on the development and commercialization
of novel medicines for patients with central nervous system (CNS) disorders, today announced receipt of a $15 million tranche under its
non-dilutive ex-US royalty-based financing (the R-Bridge Financing). This tranche of funding was triggered by the first commercial sale
of OLINVYK in China by Jiangsu Nhwa, the Company’s licensee in China. As previously announced, OLINVYK has been approved in China
for use in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative
treatments are inadequate.
The $15 million tranche is in addition to the
$28.1 million of cash and cash equivalents the Company previously reported as of June 30, 2023. As part of the R-Bridge Financing,
Trevena may receive an additional $10 million upon achievement of either a commercial or financing milestone.
The Company also announced additional expected near-term milestones:
| · | New
VOLITION Respiratory Data for OLINVYK. The Company previously reported initial topline
GI and delirium data from the ~200 patient OLINVYK VOLITION study, a real-world, open-label,
multi-site study led by clinical outcomes research experts from Cleveland Clinic and Wake
Forest Baptist Health Medical Center. Trevena expects to report new respiratory data from
the study using continuous respiratory monitoring in 3Q 2023. |
| · | OLINVYK
Abstracts Accepted at American Society of Anesthesiologists (ASA) 2023 Meeting. The Company
has three abstracts accepted for presentation at ASA, which will be held in San Francisco
from October 13th to the 17th. One abstract was selected for an
oral presentation as a top research abstract. The abstracts are embargoed until the conclusion
of the meeting and at which time they will be available at https://www.trevena.com/publications. |
| o | “ARTEMIS,
A Real-World Evidence Trial Examining the Use of Oliceridine, a Biased Agonist at the μ(Mu)
Receptor, in Patients Requiring Post-Surgical Pain Control.” With lead author Todd
L. Wandstrat, PharmD of Trevena, Inc. |
| o | “Postoperative
Vomiting With IV Oliceridine in Postoperative Recovery: A Single-group Prospective Cohort
Study” with lead author Mark Demitrack, M.D of Trevena, Inc. |
| o | “Antinociception
Versus Neurocognitive Effect of Biased Mu-opioid Receptor Oliceridine Versus Morphine- Utility
Function Analysis” with lead author Albert Dahan MD PhD of the Centre for Human
Drug Research, Leiden, the Netherlands |
| · | TRV045
Data. The Company today reported results from its Target Engagement (PainCart®) and
TMS Proof-of-Concept studies. In addition, a nonclinical study of TRV045 is ongoing, focused
on the potential of TRV045 to treat infantile spasms, a rare pediatric disorder. TRV045 is
also being studied by the NIH’s Epilepsy Therapy Screening Program as a potential disease-modifying
therapeutic for the prevention of seizures. Nonclinical data from both of these studies are
expected 2H 2023. |
| · | Trevena
to Participate in Investor Conference. The Company announces that members of management
will participate in the HC Wainwright Global Investment Conference being held in-person and
virtually in New York City on September 11-13. A link to the webcast will be available
on the Events page of the Investors section of the Company’s website at: https://www.trevena.com/investors/events-presentations/ir-calendar |
Conference Call and Webcast Information
The Company will host a conference call and webcast
with the investment community on September 6, 2023 at 8:00 a.m. Eastern Time featuring remarks by Carrie Bourdow, President
and Chief Executive Officer, Mark Demitrack, M.D., Senior Vice President and Chief Medical Officer, and Barry Shin, Chief Financial Officer.
| Title: |
Trevena Business Update
Conference Call & Webcast |
| Date: |
Wednesday, September 6, 2023 |
| Time: |
8:00 a.m. Eastern Time |
Conference
Call
Details: |
Toll-Free:1-844-825-9789
International:1-412-317-5180
Conference ID: 10178141 |
The conference call will
be webcast live from the Company’s website and will be available via the following links:
| Webcast: |
https://viavid.webcasts.com/starthere.jsp?ei=1610714&tp_key=d4c27074df |
| |
|
| |
https://www.trevena.com/investors/events-presentations/ir-calendar |
The webcast should be accessed 15 minutes prior
to the conference call start time. A replay of the webcast will be available following the conclusion of the live broadcast and will
be accessible on the Company’s website.
About OLINVYK®
(oliceridine) injection
OLINVYK is a new chemical entity approved by
the FDA in August 2020. OLINVYK contains oliceridine, an opioid, which is a Schedule II controlled substance with a high potential
for abuse similar to other opioids. It is indicated in adults for the management of acute pain severe enough to require an intravenous
opioid analgesic and for whom alternative treatments are inadequate. OLINVYK is available in 1 mg/1 mL and 2 mg/2 mL single-dose vials,
and a 30 mg/30 mL single-patient-use vial for patient-controlled analgesia (PCA). Approved PCA doses are 0.35 mg and 0.5 mg and single
doses greater than 3 mg should not be administered. The cumulative daily dose should not exceed 27 mg. Please see Important Safety Information,
including the BOXED WARNING, and full prescribing information at www.OLINVYK.com.
IMPORTANT
SAFETY INFORMATION
WARNING: ADDICTION,
ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISKS FROM CONCOMITANT USE WITH
BENZODIAZEPINES OR OTHER CENTRAL NERVOUS SYSTEM (CNS) DEPRESSANTS
ADDICTION, ABUSE,
AND MISUSE – OLINVYK exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to
overdose and death. Assess each patient’s risk before prescribing OLINVYK, and monitor all patients regularly for the development
of behaviors or conditions.
LIFE-THREATENING
RESPIRATORY DEPRESSION – Serious, life-threatening, or fatal respiratory depression may occur with use of OLINVYK. Monitor
for respiratory depression, especially during initiation of OLINVYK or following a dose increase.
NEONATAL OPIOID WITHDRAWAL
SYNDROME – Prolonged use of OLINVYK during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening
if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required
for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate
treatment will be available.
RISK FROM CONCOMITANT
USE WITH BENZODIAZEPINES OR OTHER CNS DEPRESSANTS – Concomitant use of opioids with benzodiazepines or other CNS depressants,
including alcohol, may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing for use
in patients for whom alternative treatment options are inadequate; limit dosages and durations to the minimum required; and follow patients
for signs and symptoms of respiratory depression and sedation.
INDICATIONS AND USAGE
OLINVYK is an opioid agonist indicated in adults
for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate.
LIMITATIONS OF USE
Because of the risks of addiction, abuse, and
misuse with opioids, even at recommended doses, reserve OLINVYK for use in patients for whom alternative treatment options [e.g., non-opioid
analgesics or opioid combination products]:
| · | Have
not been tolerated, or are not expected to be tolerated |
| · | Have
not provided adequate analgesia, or are not expected to provide adequate analgesia. |
The cumulative total daily dose should not exceed 27
mg, as total daily doses greater than 27 mg may increase the risk for QTc interval prolongation.
CONTRAINDICATIONS
OLINVYK is contraindicated in patients with:
| · | Significant
respiratory depression |
| · | Acute
or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment |
| · | Known
or suspected gastrointestinal obstruction, including paralytic ileus |
| · | Known
hypersensitivity to oliceridine (e.g., anaphylaxis) |
WARNINGS AND PRECAUTIONS
| · | OLINVYK
contains oliceridine, a Schedule II controlled substance, that exposes users to the risks
of addiction, abuse, and misuse. Although the risk of addiction in any individual is unknown,
it can occur in patients appropriately prescribed OLINVYK. Assess risk, counsel, and monitor
all patients receiving opioids. |
| · | Serious,
life-threatening respiratory depression has been reported with the use of opioids, even when
used as recommended, especially in patients with chronic pulmonary disease, or in elderly,
cachectic and debilitated patients. The risk is greatest during initiation of OLINVYK therapy,
following a dose increase, or when used with other drugs that depress respiration. Proper
dosing of OLINVYK is essential, especially when converting patients from another opioid product
to avoid overdose. Management of respiratory depression may include close observation, supportive
measures, and use of opioid antagonists, depending on the patient’s clinical status. |
| · | Opioids
can cause sleep-related breathing disorders including central sleep apnea (CSA) and sleep-related
hypoxemia with risk increasing in a dose-dependent fashion. In patients who present
with CSA, consider decreasing the dose of opioid using best practices for opioid taper. |
| · | Prolonged
use of opioids during pregnancy can result in withdrawal in the neonate that may be life-threatening.
Observe newborns for signs of neonatal opioid withdrawal syndrome and manage accordingly.
Advise pregnant women using OLINVYK for a prolonged period of the risk of neonatal opioid
withdrawal syndrome and ensure that appropriate treatment will be available. |
| · | Profound
sedation, respiratory depression, coma, and death may result from the concomitant use of
OLINVYK with benzodiazepines or other CNS depressants (e.g., non-benzodiazepine sedatives/hypnotics,
anxiolytics, tranquilizers, muscle relaxants, general anesthetics, antipsychotics, other
opioids, or alcohol). Because of these risks, reserve concomitant prescribing of these drugs
for use in patients for whom alternative treatment options are inadequate, prescribe the
lowest effective dose, and minimize the duration. |
| · | OLINVYK
was shown to have mild QTc interval prolongation in thorough QT studies where patients were
dosed up to 27 mg. Total cumulative daily doses exceeding 27 mg per day were
not studied and may increase the risk for QTc interval prolongation. Therefore, the cumulative
total daily dose of OLINVYK should not exceed 27 mg. |
| · | Increased
plasma concentrations of OLINVYK may occur in patients with decreased Cytochrome P450 (CYP)
2D6 function or normal metabolizers taking moderate or strong CYP2D6 inhibitors; also in
patients taking a moderate or strong CYP3A4 inhibitor, in patients with decreased CYP2D6
function who are also receiving a moderate or strong CYP3A4 inhibitor, or with discontinuation
of a CYP3A4 inducer. These patients may require less frequent dosing and should be closely
monitored for respiratory depression and sedation at frequent intervals. Concomitant use
of OLINVYK with CYP3A4 inducers or discontinuation of a moderate or strong CYP3A4 inhibitor
can lower the expected concentration, which may decrease efficacy, and may require supplemental
doses. |
| · | Cases
of adrenal insufficiency have been reported with opioid use (usually greater than one month).
Presentation and symptoms may be nonspecific and include nausea, vomiting, anorexia, fatigue,
weakness, dizziness, and low blood pressure. If confirmed, treat with physiologic replacement
doses of corticosteroids and wean patient from the opioid. |
| · | OLINVYK
may cause severe hypotension, including orthostatic hypotension and syncope in ambulatory
patients. There is increased risk in patients whose ability to maintain blood pressure has
already been compromised by a reduced blood volume or concurrent administration of certain
CNS depressant drugs (e.g., phenothiazines or general anesthetics). Monitor these patients
for signs of hypotension. In patients with circulatory shock, avoid the use of OLINVYK as
it may cause vasodilation that can further reduce cardiac output and blood pressure. |
| · | Avoid
the use of OLINVYK in patients with impaired consciousness or coma. OLINVYK should be used
with caution in patients who may be susceptible to the intracranial effects of CO2 retention,
such as those with evidence of increased intracranial pressure or brain tumors, as a reduction
in respiratory drive and the resultant CO2 retention can further increase
intracranial pressure. Monitor such patients for signs of sedation and respiratory depression,
particularly when initiating therapy. |
| · | As
with all opioids, OLINVYK may cause spasm of the sphincter of Oddi, and may cause increases
in serum amylase. Monitor patients with biliary tract disease, including acute pancreatitis,
for worsening symptoms. |
| · | OLINVYK
may increase the frequency of seizures in patients with seizure disorders and may increase
the risk of seizures in vulnerable patients. Monitor patients with a history of seizure disorders
for worsened seizure control. |
| · | Do
not abruptly discontinue OLINVYK in a patient physically dependent on opioids. Gradually
taper the dosage to avoid a withdrawal syndrome and return of pain. Avoid the use of mixed
agonist/antagonist (e.g., pentazocine, nalbuphine, and butorphanol) or partial agonist (e.g.,
buprenorphine) analgesics in patients who are receiving OLINVYK, as they may reduce the analgesic
effect and/or precipitate withdrawal symptoms. |
| · | OLINVYK
may impair the mental or physical abilities needed to perform potentially hazardous activities
such as driving a car or operating machinery. |
| · | Although
self-administration of opioids by patient-controlled analgesia (PCA) may allow each patient
to individually titrate to an acceptable level of analgesia, PCA administration has resulted
in adverse outcomes and episodes of respiratory depression. Health care providers and family
members monitoring patients receiving PCA analgesia should be instructed in the need for
appropriate monitoring for excessive sedation, respiratory depression, or other adverse effects
of opioid medications. |
ADVERSE REACTIONS
Adverse reactions are described in greater detail
in the Prescribing Information.
The most common (incidence ≥10%) adverse reactions
in Phase 3 controlled clinical trials were nausea, vomiting, dizziness, headache, constipation, pruritus, and hypoxia.
MEDICAL INFORMATION
For medical inquiries or to report an adverse
event, other safety-related information or product complaints for a company product, please contact the Trevena Medical Information Contact
Center at 1-844-465-4686 or email MedInfo@Trevena.com.
You are encouraged to report suspected adverse
events of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088.
Please see Full Prescribing Information,
including Boxed Warning.
About TRV045
TRV045 is a novel, selective
sphingosine-1-phosphate subtype 1 (S1P1) receptor modulator being developed as a potential treatment for acute and chronic
neuropathic pain secondary to diabetic peripheral neuropathy. Through a collaboration with the National Institutes of Health, Trevena
is also exploring TRV045 as a potential treatment for epilepsy.
S1P receptors are located
throughout the body, including the central nervous system, where they are believed to play a role in modulating neurotransmission and
membrane excitability.
Trevena's discovery
efforts have identified a family of compounds that are highly selective for the S1P1 receptor. TRV045 reversed thermal
hyperalgesia, a measure of neuropathic pain, in nonclinical models of diabetic peripheral neuropathy and chemotherapy-induced peripheral
neuropathy. TRV045 was not associated with lymphopenia and produced no changes in blood pressure, heart rate, or respiratory function
at or above pharmacologically active doses in nonclinical studies. TRV045 is an investigational product and is not yet approved by the
FDA.
About Epilepsy
Epilepsy, one of the most common neurological
diseases in the world, is a chronic disorder characterized by recurrent seizures. Epilepsy is defined as having two or more unprovoked
seizures separated by at least 24 hours or after one seizure with a high risk of more.
A seizure is a sudden surge of electrical activity
in the brain caused by complex chemical changes that occur in nerve cells. Usually, there is a balance of cells that either encourage
or stop other brain cells from sending messages. A seizure occurs when there may be too much or too little electrical activity in the
brain causing an imbalance. Seizures are a symptom of many different disorders that can affect the brain. Nearly 50 million people suffer
from epilepsy worldwide, including 3 million adults and 470,000 children in the U.S. 150,000 new cases of epilepsy are reported in the
United States each year. According to the CDC, 56% of adults living with diagnosed epilepsy continue to have seizures.
About Diabetic Neuropathic Pain
Diabetic neuropathy is a common complication
of both type 1 and type 2 diabetes, with pain in the extremities being one of the main symptoms. Other symptoms may include numbness,
tingling, allodynia and hyperalgesia. Diabetic neuropathic pain is usually characterized as moderate to severe in nature and can
substantially affect patients’ quality of life as well as their social and psychological well-being.
Approximately 25% of people with diabetes are
affected by DNP, equaling over 5 million people in the U.S. During their lifetime, approximately 50% to 70% of diabetic patients
may experience symptoms of DNP.
Forward-Looking Statements
Any statements in this press release about future
expectations, plans and prospects for the Company, including statements about the Company’s strategy, future operations, clinical
development and trials of its therapeutic candidates, plans for potential future product candidates and other statements containing the
words “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,”
“plan,” “predict,” “project,” “suggest,” “target,” “potential,”
“will,” “would,” “could,” “should,” “continue,” and similar expressions,
constitute forward-looking statements within the meaning of The Private Securities Litigation Reform Act of 1995. Actual results may
differ materially from those indicated by such forward-looking statements as a result of various important factors, including: the status,
timing, costs, results and interpretation of the Company’s clinical trials or any future trials of any of the Company’s investigational
drug candidates; the uncertainties inherent in conducting clinical trials; expectations for regulatory interactions, submissions and
approvals, including the Company’s assessment of discussions with FDA; available funding; uncertainties related to the Company’s
intellectual property; other matters that could affect the availability or commercial potential of the Company’s therapeutic candidates
and approved product; and other factors discussed in the Risk Factors set forth in the Company’s Annual Report on Form 10-K
and Quarterly Reports on Form 10-Q filed with the Securities and Exchange Commission (SEC) and in other filings the Company makes
with the SEC from time to time. In addition, the forward-looking statements included in this press release represent the Company’s
views only as of the date hereof. The Company anticipates that subsequent events and developments may cause the Company’s views
to change. However, while the Company may elect to update these forward-looking statements at some point in the future, it specifically
disclaims any obligation to do so, except as may be required by law.
About Trevena
Trevena, Inc. is a biopharmaceutical company
focused on the development and commercialization of innovative medicines for patients with CNS disorders. The Company has one approved
product in the United States, OLINVYK® (oliceridine) injection, indicated in adults for the management of acute pain
severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. The Company’s novel
pipeline is based on Nobel Prize winning research and includes three differentiated investigational drug candidates: TRV045 for diabetic
neuropathic pain and epilepsy, TRV250 for the acute treatment of migraine and TRV734 for maintenance treatment of opioid use disorder.
For more information, please visit www.Trevena.com
About
Jiangsu Nhwa:
Jiangsu
Nhwa Pharmaceutical Co., Ltd. (SZ002262), founded in 1978, is a leading CNS company in China. Over the past 40 years, Nhwa is exclusively
dedicated to developing innovative and differentiated pipeline in the areas of anesthesia, analgesia, psychiatry and neurology via in-house
R&D and global partnership.
As a fully
integrated pharmaceutical company with more than 4000 employees, Nhwa has comprehensive capabilities in research, clinical development,
manufacturing and commercialization of CNS drugs. In recent years, Nhwa has further strengthened its leadership in CNS field in China
by providing the services of precision diagnosis of CNS disorders (Shanghai N-yuen Biotechnology Company), and investing the largest
Chinese CNS internet health platform (Happy Mood).
About R-Bridge (CBC Group)
CBC
Group is Asia’s largest and most active healthcare-dedicated investment firm with over US$5 billion AUM, focused on platform-building,
buyout opportunities, and alternative financing across three core areas: pharmaceutical & biotech, medtech, and healthcare services.
CBC has a leading team of investment, industry and portfolio management professionals, headquartered in Singapore with offices in New
York, Shanghai, Beijing, and Hong Kong and presence in Boston, San Diego, San Francisco and Tokyo.
Founded in February 2020, R-Bridge Healthcare
Fund is an affiliate of CBC Group and it is dedicated in providing alternative, non-dilutive financing backed by royalties, revenue interest
and other cash flows generated by the sale of healthcare products and services in China, the first of its kind for the asset class and
the region. R-Bridge provides additional sources of capital to leading healthcare companies to continue their extraordinary growth trajectories,
commercializing their products and services in China and on a global scale.
For more information, please contact:
Investor Contact:
Dan Ferry
Managing Director
LifeSci Advisors, LLC
daniel@lifesciadvisors.com
(617) 430-7576
Company Contact:
Bob Yoder
SVP and Chief Business Officer
Trevena, Inc.
(610) 354-8840
v3.23.2
Cover
|
Sep. 06, 2023 |
| Cover [Abstract] |
|
| Document Type |
8-K
|
| Amendment Flag |
false
|
| Document Period End Date |
Sep. 06, 2023
|
| Entity File Number |
001-36193
|
| Entity Registrant Name |
TREVENA, INC.
|
| Entity Central Index Key |
0001429560
|
| Entity Tax Identification Number |
26-1469215
|
| Entity Incorporation, State or Country Code |
DE
|
| Entity Address, Address Line One |
955 Chesterbrook Boulevard
|
| Entity Address, Address Line Two |
Suite 110
|
| Entity Address, City or Town |
Chesterbrook
|
| Entity Address, State or Province |
PA
|
| Entity Address, Postal Zip Code |
19087
|
| City Area Code |
610
|
| Local Phone Number |
354-8840
|
| Written Communications |
false
|
| Soliciting Material |
false
|
| Pre-commencement Tender Offer |
false
|
| Pre-commencement Issuer Tender Offer |
false
|
| Title of 12(b) Security |
Common Stock, $0.001 par value
|
| Trading Symbol |
TRVN
|
| Security Exchange Name |
NASDAQ
|
| Entity Emerging Growth Company |
false
|
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 2 such as Street or Suite number
| Name: |
dei_EntityAddressAddressLine2 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Section 14a
-Number 240
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
Trevena (NASDAQ:TRVN)
Historical Stock Chart
From Aug 2024 to Sep 2024

Trevena (NASDAQ:TRVN)
Historical Stock Chart
From Sep 2023 to Sep 2024
