false 0001661998 0001661998 2024-12-10 2024-12-10
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): December 10, 2024
Q32 Bio Inc.
(Exact name of Registrant as Specified in Its Charter)
|
|
|
|
|
| Delaware |
|
001-38433 |
|
47-3468154 |
(State or Other Jurisdiction
of Incorporation) |
|
(Commission File Number) |
|
(IRS Employer
Identification No.) |
|
|
|
| 830 Winter Street |
|
|
| Waltham, Massachusetts |
|
02451 |
| (Address of Principal Executive Offices) |
|
(Zip Code) |
Registrant’s Telephone Number, Including Area Code: 781 999-0232
N/A
(Former Name or Former Address, if Changed Since Last Report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
|
|
|
|
|
|
Title of each class
|
|
Trading
Symbol(s) |
|
Name of each exchange
on which registered |
| Common stock, par value $0.0001 per share |
|
QTTB |
|
The Nasdaq Global Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§ 230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§ 240.12b-2 of this chapter).
Emerging growth company ☐
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
| Item 7.01 |
Regulation FD Disclosure. |
On December 10, 2024, Q32 Bio Inc. (the “Company”) issued a press release titled “Q32 Bio Provides Bempikibart Program Update, Including Next Steps for Advancing Alopecia Areata Development Program.” A copy of the press release in connection with the announcement is being furnished as Exhibit 99.1 to this Current Report on Form 8-K.
The information in this Current Report on Form 8-K (including Exhibit 99.1 attached hereto) is intended to be furnished and shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”) or otherwise subject to the liabilities of that section, nor shall it be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act, except as expressly set forth by specific reference in such filing.
On December 10, 2024, the Company announced topline results from the SIGNAL-AA Phase 2a signal finding clinical trial evaluating bempikibart (ADX-914) in patients with alopecia areata (“AA”) and topline results from the SIGNAL-AD Phase 2a clinical trial evaluating bempikibart in atopic dermatitis (“AD”). The Company also updated its corporate deck, a copy of which is filed as Exhibit 99.2 to this Current Report on Form 8-K and incorporated herein by reference.
Topline Results from SIGNAL-AA Phase 2a Clinical Trial
SIGNAL-AA is a Phase 2a, randomized, double-blind, placebo-controlled, multi-center clinical trial evaluating bempikibart in adult patients with severe and very severe AA (baseline Severity of Alopecia Tool (SALT) scores of 50-100) treated over 24 weeks, with follow-up through 36 weeks. The study is being conducted to evaluate the efficacy and safety of bempikibart 200 mg administered subcutaneously (SC), every-other-week (Q2W) compared to placebo. A total of 44 patients were enrolled in the trial with a primary endpoint of the mean relative percent change in SALT score at 24 weeks compared with baseline.
Following database lock, one site was excluded from the efficacy analysis based on marked protocol violations of entry criteria. This resulted in the removal of three placebo patients, rendering the planned statistical analyses for the primary endpoint inappropriate due to the reduced sample size. On a post-hoc analysis of the remaining per-protocol population of patients with AA (n=27), bempikibart demonstrated an improvement in hair re-growth compared to placebo:
| |
• |
|
At week 24: patients treated with bempikibart showed a mean reduction in SALT score of 16% in the bempikibart group vs a reduction of 2% in the placebo group. A Wilcoxon Rank Sum test yielded a p-value of 0.045. |
| |
• |
|
At week 24: 9% of bempikibart patients in the trial achieved a SALT-20 (SALT score less than or equal to 20) compared to 0% in placebo. |
| |
• |
|
At week 26: 13% of bempikibart patients achieved SALT-20 compared 0% in placebo. |
Bempikibart was observed to be safe and well tolerated in the SIGNAL-AA trial. There were no serious adverse events (SAE) or Grade 3 or higher adverse events related to treatment.
The Company plans to enroll approximately 20 additional patients in a Part B expansion of the SIGNAL-AA Phase 2a clinical trial to further evaluate bempikibart in AA, including a loading regimen. The Company will defer enrollment into the planned Phase 2 clinical trial of ADX-097 in ANCA-Associated Vasculitis (AAV), previously expected to begin in 2025, to focus efforts on continued enrollment in the ongoing bempikibart AA and ADX-097 renal basket Phase 2 clinical trials.
Topline Results from SIGNAL-AD Phase 2a Clinical Trial
SIGNAL-AD is a two-part Phase 2a, randomized, double-blind, placebo-controlled, multi-center clinical trial evaluating bempikibart in adult patients with persistent, moderate-to-severe AD. Part A (n=15) was conducted to evaluate safety, pharmacokinetics (PK), and to enable dose selection for Part B of the clinical trial. Part A was randomized 2:1 between bempikibart and placebo in each of two dose cohorts of 2mg/kg or 3mg/kg Q2W SC for 12 weeks.
In Part A, at week 14, improvement in average EASI score from baseline was 58% in patients treated with 2mg/kg Q2W SC and 84% in patients treated at 3mg/kg Q2W SC, and 72% on a pooled basis, compared to 38% in patients treated with placebo.
In Part B, which evaluated both efficacy and safety of bempikibart compared to placebo, patients were enrolled 1:1 in the bempikibart 200 mg Q2W SC (n=52) and placebo (n=54) arms for 12 weeks of treatment. The primary endpoint is the mean percent change from baseline to week 14 in the Eczema Area and Severity Index (EASI) score. At week 14, data from Part B demonstrated that patients treated with bempikibart showed a 74% improvement in average EASI from baseline, compared to 76% for the placebo group (p= not statistically significant). Results of the primary endpoint were generally consistent when stratified for pre-specified baseline entry criteria. Bempikibart was observed to be safe and well tolerated in the SIGNAL-AD trial. There were no serious adverse events (SAE) or Grade 3 or higher adverse events related to treatment. The Company plans to conduct a review of the SIGNAL-AD results.
Biomarker Results in SIGNAL-AD and SIGNAL-AA:
Across SIGNAL-AD and SIGNAL-AA, bempikibart at 200mg Q2W SC demonstrated favorable PK and target engagement as demonstrated by substantial reductions in biomarkers of Th2 and Th1. These results include:
| |
• |
|
A reduction in Th2 biomarkers, including TARC, IgE and eosinophils, which was consistent with the type of biomarker impact previously observed with other agents that have demonstrated utility in atopic dermatitis, such as IL-4Rα, IL-13 and OX40 ligand-targeted agents. |
| |
• |
|
An expected modulation of T-cells, with a 20-30% reduction, consistent with target engagement and IL-7Rα blockade. |
The Company believes these results demonstrate that bempikibart is a potent inhibitor of both TSLP and IL-7 signaling as evidenced by robust changes in both Th2 biomarkers and T-cells. The Company believes the mechanism of action of bempikibart has the potential to be active in other Th2 and Th1 driven diseases, including asthma, COPD, ulcerative colitis (UC), rheumatoid arthritis (RA), celiac disease, multiple sclerosis (MS) and others.
Forward-Looking Statements
This Current Report on Form 8-K contains forward-looking statements within the meaning of the U.S. Private Securities Litigation Reform Act of 1995, as amended, and other federal securities laws,. Any statements contained herein which do not describe historical facts, including, among others, our beliefs, observations, expectations and assumptions regarding the topline data from the SIGNAL-AA Phase 2a and the safety, tolerability, clinical activity including biomarker data, potential efficacy and potential benefits of bempikibart; plans and expectations for Part B of the SIGNAL-AA Phase 2a clinical trial are forward-looking statements, which involve risks and uncertainties that could cause actual results to differ materially from those discussed in such forward-looking statements.
Forward-looking statements generally include statements that are predictive in nature and depend upon or refer to future events or conditions, and include words such as “may,” “will,” “should,” “would,” “expect,” “anticipate,” “plan,” “likely,” “believe,” “estimate,” “project,” “intend,” and other similar expressions among others. Statements that are not historical facts are forward-looking statements. Forward-looking statements are based on management’s current beliefs and assumptions, which are subject to risks and uncertainties and are not guarantees of future performance. Such risks and uncertainties include, among others, the risk that additional data, or the results of ongoing data analyses, may not support our current beliefs and expectations for bempikibart; future clinical studies, including the Part B of the SIGNAL-AA Phase 2a clinical trial, may not be completed in a timely manner or at all, might be more costly than expected or might not yield anticipated results, the Company may need additional funding to complete its clinical studies, which may not be available on favorable terms or at all, and such other risks and uncertainties identified in the Company’s periodic, current and other filings with the U.S. Securities and Exchange Commission, including its Quarterly Report on Form 10-Q for the quarter ended September 30, 2024 and any subsequent filings with the Commission, which are available at the SEC’s website at www.sec.gov. Any such risks and uncertainties could materially and adversely affect the Company’s results of operations and its cash flows, which would, in turn, have a significant and adverse impact on the Company’s stock price. We caution you not to place undue reliance on any forward-looking statements, which speak only as of the date they are made. The Company disclaims any obligation to publicly update or revise any such statements to reflect any change in expectations or in events, conditions or circumstances on which any such statements may be based, or that may affect the likelihood that actual results will differ from those set forth in the forward-looking statements.
| Item 9.01 |
Financial Statements and Exhibits. |
(d) Exhibits.
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
|
|
|
|
|
|
|
|
|
|
|
|
Q32 BIO INC. |
|
|
|
|
| Date: December 11, 2024 |
|
|
|
By: |
|
/s/ Jodie Morrison |
|
|
|
|
Name: Title: |
|
Jodie Morrison
Chief Executive Officer |
Exhibit 99.1

Q32 Bio Provides Bempikibart Program Update, Including Next Steps for Advancing Alopecia Areata
Development Program
— SIGNAL-AA demonstrated encouraging clinical activity of
bempikibart in patients with alopecia areata (AA), including improvement from baseline on SALT score and meaningful achievement of SALT-20 response —
— SIGNAL-AD Phase 2a clinical trial in atopic dermatitis demonstrated promising findings in
Part A but did not meet primary endpoint in Part B —
— Across both trials, bempikibart was observed to be safe and well
tolerated; demonstrated potent IL-7 and TSLP inhibition via changes in both Th2 biomarkers and T-cells, and desired target engagement —
— Based on these results, Company plans to advance bempikibart in patients with AA —
WALTHAM, Mass.— December 10, 2024 – Q32 Bio Inc. (Nasdaq: QTTB) (“Q32 Bio”), a clinical stage biotechnology
company focused on developing biologic therapeutics to restore immune homeostasis, today announced topline results from the SIGNAL-AA Phase 2a signal finding clinical trial evaluating bempikibart (ADX-914), which identified encouraging clinical activity in patients with alopecia areata (AA). The Company plans to expand the SIGNAL-AA Phase 2a clinical trial and enroll
additional patients evaluating bempikibart in AA.
“We are pleased with the emerging signals observed in the
SIGNAL-AA Phase 2a clinical trial and based upon these, the positive biomarker data and well tolerated safety profile observed across both trials, we plan to enroll additional patients into the SIGNAL-AA clinical trial to further explore the clinical effects of bempikibart in this patient population. We believe bempikibart has the potential to be an important new treatment option in a disease needing new
and safer alternatives to currently approved agents,” said Jodie Morrison, Chief Executive Officer of Q32 Bio. “We are disappointed that the SIGNAL-AD trial did not achieve its primary endpoint.
Based upon the findings, including the high placebo rate, we plan to conduct a review to better understand the results.”
“Results from our
analysis of SIGNAL-AA showed clinically meaningful activity and a safety profile that we believe is differentiated from the currently approved therapies for AA. We are encouraged by our findings from this
clinical trial, and we look forward to advancing bempikibart as a potential treatment for AA,” said Jason Campagna, M.D., Ph.D., Chief Medical Officer of Q32 Bio. “On behalf of Q32 Bio, I want to express my gratitude to the patients, their
caregivers, and clinical trial sites that participated across both our bempikibart Phase 2a trials.”
The Company is also providing an update on the SIGNAL-AD clinical trial in patients with atopic dermatitis (AD). Although the Company is reporting promising findings in Part A, the trial did not meet its primary endpoint in Part B. Q32 Bio plans to conduct a
review of the results.
Topline Results from SIGNAL-AA Phase 2a Clinical Trial:
SIGNAL-AA is a Phase 2a, randomized, double-blind, placebo-controlled, multi-center clinical trial evaluating
bempikibart in adult patients with severe and very severe AA (baseline Severity of Alopecia Tool (SALT) scores of 50-100) treated over 24 weeks, with follow-up through
36 weeks. The study is being conducted to evaluate the efficacy and safety of bempikibart 200 mg administered subcutaneously (SC), every-other-week (Q2W) compared to placebo. A total of 44 patients were enrolled in the trial with a primary endpoint
of the mean relative percent change in SALT score at 24 weeks compared with baseline.
Following database lock, one site was excluded from the efficacy
analysis based on marked protocol violations of entry criteria. This resulted in the removal of three placebo patients, rendering the planned statistical analyses for the primary endpoint inappropriate due to the reduced sample size. On a post-hoc analysis of the remaining per-protocol population of patients with AA (n=27), bempikibart demonstrated an improvement in hair
re-growth compared to placebo:
| |
• |
|
At week 24: patients treated with bempikibart showed a mean reduction in SALT score of 16% in the bempikibart
group vs a reduction of 2% in the placebo group. A Wilcoxon Rank Sum test yielded a p-value of 0.045. |
| |
• |
|
At week 24: 9% of bempikibart patients in the trial achieved a SALT-20
(SALT score less than or equal to 20) compared to 0% in placebo. |
| |
• |
|
At week 26: 13% of bempikibart patients achieved SALT-20 compared 0% in
placebo. |
Bempikibart was observed to be safe and well tolerated in the SIGNAL-AA trial. There
were no serious adverse events (SAE) or Grade 3 or higher adverse events related to treatment.
“Advancing bempikibart in AA is supported by
preclinical data demonstrating the potential of IL-7Rα inhibition in this disease, and now the resulting data from SIGNAL-AA demonstrated the clinical potential of
an IL-7Rα inhibitor in AA. I am encouraged by the biomarker data that provide evidence of biological activity, the safety profile of bempikibart, and the clinical signal of hair regrowth in
patients,” said Brett King, M.D., Ph.D., of Dermatology Physicians of Connecticut, and former Associate Professor of Dermatology, Yale University School of Medicine. “I believe these clinical results are promising and warrant further
advancement to expand upon these findings.”
Q32 Bio plans to enroll approximately 20 additional patients in a Part B expansion of the SIGNAL-AA Phase 2a clinical trial to further evaluate bempikibart in AA, including a loading regimen. The Company will defer enrollment into the planned Phase 2 clinical trial of
ADX-097 in ANCA-Associated Vasculitis (AAV), previously expected to begin in 2025, to focus efforts on continued enrollment in the ongoing bempikibart AA and ADX-097
renal basket Phase 2 clinical trials.
Topline Results from SIGNAL-AD Phase 2a Clinical Trial:
SIGNAL-AD is a two-part Phase 2a, randomized, double-blind, placebo-controlled,
multi-center clinical trial evaluating bempikibart in adult patients with persistent, moderate-to-severe AD. Part A (n=15) was conducted to evaluate safety,
pharmacokinetics (PK), and to enable dose selection for Part B of the clinical trial. Part A was randomized 2:1 between bempikibart and placebo in each of two dose cohorts of 2mg/kg or 3mg/kg Q2W SC for 12 weeks.
In Part A, at week 14, improvement in average EASI score from baseline was 58% in patients treated with
2mg/kg Q2W SC and 84% in patients treated at 3mg/kg Q2W SC, and 72% on a pooled basis, compared to 38% in patients treated with placebo.
In Part B, which
evaluated both efficacy and safety of bempikibart compared to placebo, patients were enrolled 1:1 in the bempikibart 200 mg Q2W SC (n=52) and placebo (n=54) arms for 12 weeks of treatment. The primary endpoint is the mean percent change from
baseline to week 14 in the Eczema Area and Severity Index (EASI) score. At week 14, data from Part B demonstrated that patients treated with bempikibart showed a 74% improvement in average EASI from baseline, compared to 76% for the placebo group
(p= not statistically significant). Results of the primary endpoint were generally consistent when stratified for pre-specified baseline entry criteria. Bempikibart was observed to be safe and well tolerated
in the SIGNAL-AD trial. There were no serious adverse events (SAE) or Grade 3 or higher adverse events related to treatment. Q32 Bio plans to conduct a review of the
SIGNAL-AD results.
Biomarker Results in SIGNAL-AD and SIGNAL-AA:
Across SIGNAL-AD and
SIGNAL-AA, bempikibart at 200mg Q2W SC demonstrated favorable PK and target engagement as demonstrated by substantial reductions in biomarkers of Th2 and Th1. These results include:
| |
• |
|
A reduction in Th2 biomarkers, including TARC, IgE and eosinophils, which was consistent with the type of
biomarker impact previously observed with other agents that have demonstrated utility in atopic dermatitis, such as IL-4Rα, IL-13 and OX40 ligand-targeted agents.
|
| |
• |
|
An expected modulation of T-cells, with a
20-30% reduction, consistent with target engagement and IL-7Rα blockade. |
Q32 Bio believes these results demonstrate that bempikibart is a potent inhibitor of both TSLP and IL-7 signaling as
evidenced by robust changes in both Th2 biomarkers and T-cells. The Company believes the mechanism of action of bempikibart has the potential to be active in other Th2 and Th1 driven diseases, including
asthma, COPD, ulcerative colitis (UC), rheumatoid arthritis (RA), celiac disease, multiple sclerosis (MS) and others.
“These impressive biomarker
data represent a meaningful advancement in the clinical understanding of how inhibition of IL-7Rα can be leveraged to treat autoimmune and inflammatory diseases,” said Shelia Violette, Ph.D., Co-Founder and Chief Scientific Officer of Q32 Bio. “Based upon its observed mechanism of action, bempikibart continues to show strong potential as an IL-7Rα
inhibitor to treat AA and other diseases.”
The Company has published an updated investor presentation with additional details regarding the bempikibart
update for review by interested parties. The updated presentation can be found on the company website at www.Q32Bio.com under Investors & Media.
About Q32 Bio
Q32 Bio is a clinical stage biotechnology
company developing biologic therapeutics targeting potent regulators of the innate and adaptive immune systems to re-balance immunity in autoimmune and inflammatory diseases. Q32 Bio’s lead programs,
focused on the IL-7 / TSLP receptor pathways and complement system, address immune dysregulation to help patients take back control of their lives.
Q32 Bio’s program for adaptive immunity, bempikibart (ADX-914), is a fully human
anti-IL-7Rα antibody that re-regulates adaptive immune function for the treatment of autoimmune diseases being evaluated in
a Phase 2 program. The IL-7 and TSLP pathways have been genetically and biologically implicated in driving several T cell-mediated pathological processes in numerous autoimmune diseases. Q32 Bio’s program
for innate immunity, ADX-097, being evaluated in a Phase 2 program, is based on a novel platform enabling tissue-targeted regulation of the complement system without long-term systemic blockade – a key
differentiator versus current complement therapeutics.
For more information, visit www.Q32Bio.com.
Availability of Other Information About Q32 Bio
Investors and others should note that we communicate with our investors and the public using our company website www.Q32Bio.com, including, but not
limited to, company disclosures, investor presentations and FAQs, Securities and Exchange Commission filings, press releases, public conference call transcripts and webcast transcripts, as well as on X (formerly Twitter) and LinkedIn. The
information that we post on our website or on X or LinkedIn could be deemed to be material information. As a result, we encourage investors, the media and others interested to review the information that we post there on a regular basis. The
contents of our website or social media shall not be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended.
Forward-Looking Statements
This communication contains
forward-looking statements within the meaning of the U.S. Private Securities Litigation Reform Act of 1995, as amended, and other federal securities laws. Any statements contained herein which do not describe historical facts, including, among
others, our beliefs, observations, expectations and assumptions regarding the topline data from the SIGNAL-AA Phase 2a and the safety, tolerability, clinical activity including biomarker data, potential
efficacy and potential benefits of bempikibart; plans and expectations for Part B of the SIGNAL-AA Phase 2a clinical trial are forward-looking statements, which involve risks and uncertainties that could cause
actual results to differ materially from those discussed in such forward-looking statements.
Forward-looking statements are based on management’s current beliefs and assumptions, which are subject
to risks and uncertainties and are not guarantees of future performance. Such risks and uncertainties include, among others, the risk that additional data, or the results of ongoing data analyses, may not support our current beliefs and
expectations for bempikibart, future clinical studies, including the Part B of the SIGNAL-AA Phase 2a clinical trial, may not be completed in a timely manner or at all, might be more costly than expected or
might not yield anticipated results, the Company may need additional funding to complete its clinical studies, which may not be available on favorable terms or at all, and such other risks and uncertainties identified in the Company’s periodic,
current and other filings with the U.S. Securities and Exchange Commission, including its Quarterly Report on Form 10-Q for the quarter ended September 30, 2024 and any subsequent filings with the
Commission, which are available at the SEC’s website at www.sec.gov. Any such risks and uncertainties could materially and adversely affect the Company’s results of operations and its cash flows, which would, in turn, have a
significant and adverse impact on the Company’s stock price. We caution you not to place undue reliance on any forward-looking statements, which speak only as of the date they are made. The Company disclaims any obligation to publicly
update or revise any such statements to reflect any change in expectations or in events, conditions or circumstances on which any such statements may be based, or that may affect the likelihood that actual results will differ from those set forth in
the forward-looking statements.
Contacts:
Investors:
Brendan Burns
Media: Sarah Sutton
Argot Partners
212.600.1902
Q32Bio@argotpartners.com

Exhibit 99.2 Building The Future of Immune Therapeutics Company Overview
December 2024
Forward Looking Statements This presentation has been prepared by Q32
Bio Inc. (“we”, “us,” “our,” “Q32” or the “Company”) and is made for informational purposes only. The information set forth herein does not purport to be complete or contain all of the
information you may desire. Statements contained herein are made as of the date of this presentation unless stated otherwise, and this presentation shall not under any circumstances create an implication that the information contained herein is
correct as of any time after such date or that information will be updated or revised to reflect information that subsequently becomes available or changes occurring after the date hereof. This presentation contains forward-looking statements within
the meaning of the U.S. Private Securities Litigation Reform Act of 1995. Forward-looking statements can be identified by words such as “may,” “will,” “should,” “would,” “expect,”
“anticipate,” “plan,” “likely,” “believe,” “estimate,” “project,” “intend,” “potential,” and similar expressions regarding future periods. These
forward-looking statements include, but are not limited to, our beliefs, observations, expectations and assumptions regarding the topline data from the SIGNAL-AA Phase 2a and the safety, tolerability, clinical activity including biomarker data,
potential efficacy and potential benefits of bempikibart, plans and expectations for Part B of the SIGNAL-AA Phase 2a clinical trial statements regarding expected cash and the sufficiency of the Company’s cash to fund operations into mid-
2026, the expectations surrounding the potential, safety, efficacy, and regulatory and clinical progress of Q32’s product candidates, including bempikibart and ADX-097, and anticipated milestones, data readouts and timing, among others.
Statements that are not historical facts are forward-looking statements. Forward-looking statements are based on current beliefs and assumptions that are subject to risks and uncertainties and are not guarantees of future performance. Actual results
could differ materially from those contained in any forward-looking statement as a result of various factors, including, without limitation: the Company’s need for additional funding, which may not be available; failure to identify additional
product candidates and develop or commercialize marketable products; the early stage of the Company’s development efforts; potential unforeseen events during clinical trials could cause delays or other adverse consequences; risks relating to
the regulatory approval process; interim, topline and preliminary data may change as more patient data become available, and are subject to audit and verification procedures that could result in material changes in the final data; Q32’s
product candidates may cause serious adverse side effects; inability to maintain our collaborations, or the failure of these collaborations; our reliance on third parties, including for the manufacture of materials for our research programs,
preclinical and clinical studies; failure to obtain U.S. or international marketing approval; ongoing regulatory obligations; effects of significant competition; unfavorable pricing regulations, third-party reimbursement practices or healthcare
reform initiatives; product liability lawsuits; securities class action litigation; the impact of the COVID-19 pandemic and general economic conditions on our business and operations, including our preclinical studies and clinical trials; the
possibility of system failures or security breaches; risks relating to intellectual property and our ability to protect our patents and other proprietary rights; significant costs incurred as a result of operating as a public company; as well as
those risk and uncertainties set forth more fully under the caption “Risk Factors” in our Quarterly Report on Form 10-Q for the quarter ended September 30, 2024, as well as other risks detailed in our subsequent filings with the United
States Securities and Exchange Commission. Any forward-looking statement made by us is based only on information currently available to us and speaks only as of the date on which it is made. We undertake no obligation to publicly update any
forward-looking statement, whether written or oral, that may be made from time to time, whether as a result of new information, future developments or otherwise. Certain information contained in this presentation relates to or is based on studies,
publications, analyses, surveys and other data obtained from third-party sources and the Company’s own internal estimates and research. While the Company believes these third-party sources to be reliable as of the date of this presentation, it
has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. In addition, all of the market data included in this presentation involves a
number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Finally, while we believe our own internal research is reliable, such research may not have been verified by any independent
source. 2
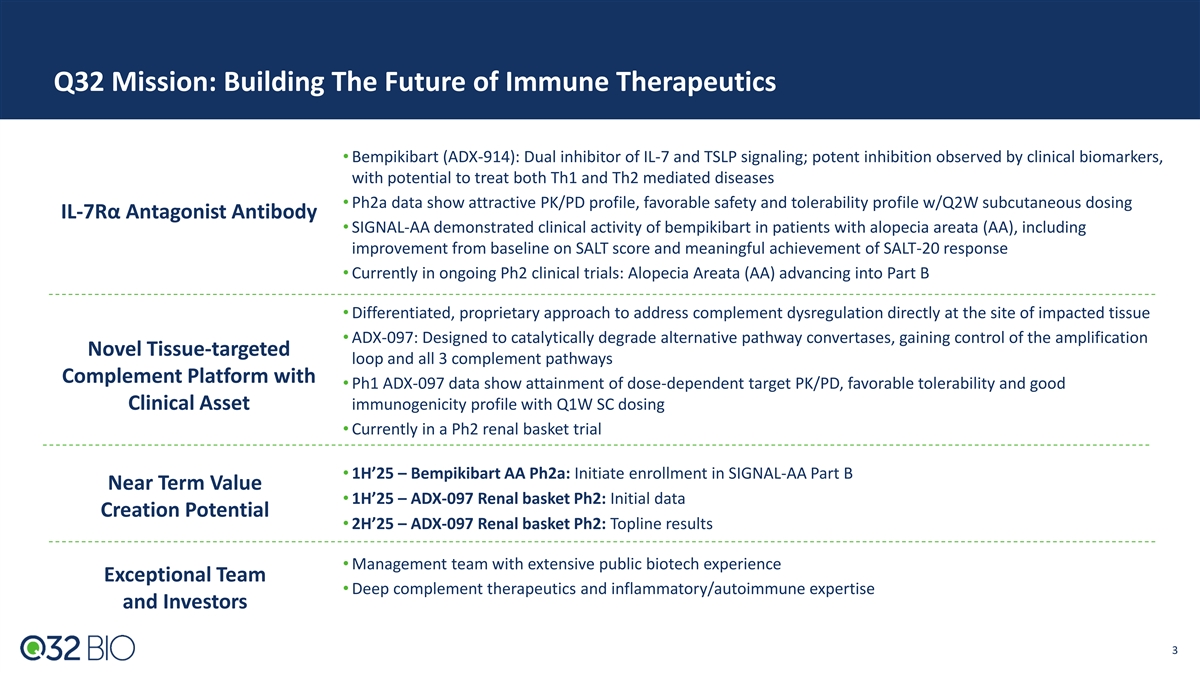
Q32 Mission: Building The Future of Immune Therapeutics •
Bempikibart (ADX-914): Dual inhibitor of IL-7 and TSLP signaling; potent inhibition observed by clinical biomarkers, with potential to treat both Th1 and Th2 mediated diseases • Ph2a data show attractive PK/PD profile, favorable safety and
tolerability profile w/Q2W subcutaneous dosing IL-7Rα Antagonist Antibody • SIGNAL-AA demonstrated clinical activity of bempikibart in patients with alopecia areata (AA), including improvement from baseline on SALT score and meaningful
achievement of SALT-20 response • Currently in ongoing Ph2 clinical trials: Alopecia Areata (AA) advancing into Part B • Differentiated, proprietary approach to address complement dysregulation directly at the site of impacted tissue
• ADX-097: Designed to catalytically degrade alternative pathway convertases, gaining control of the amplification Novel Tissue-targeted loop and all 3 complement pathways Complement Platform with • Ph1 ADX-097 data show attainment of
dose-dependent target PK/PD, favorable tolerability and good Clinical Asset immunogenicity profile with Q1W SC dosing • Currently in a Ph2 renal basket trial • 1H’25 – Bempikibart AA Ph2a: Initiate enrollment in SIGNAL-AA
Part B Near Term Value • 1H’25 – ADX-097 Renal basket Ph2: Initial data Creation Potential • 2H’25 – ADX-097 Renal basket Ph2: Topline results • Management team with extensive public biotech experience
Exceptional Team • Deep complement therapeutics and inflammatory/autoimmune expertise and Investors 3
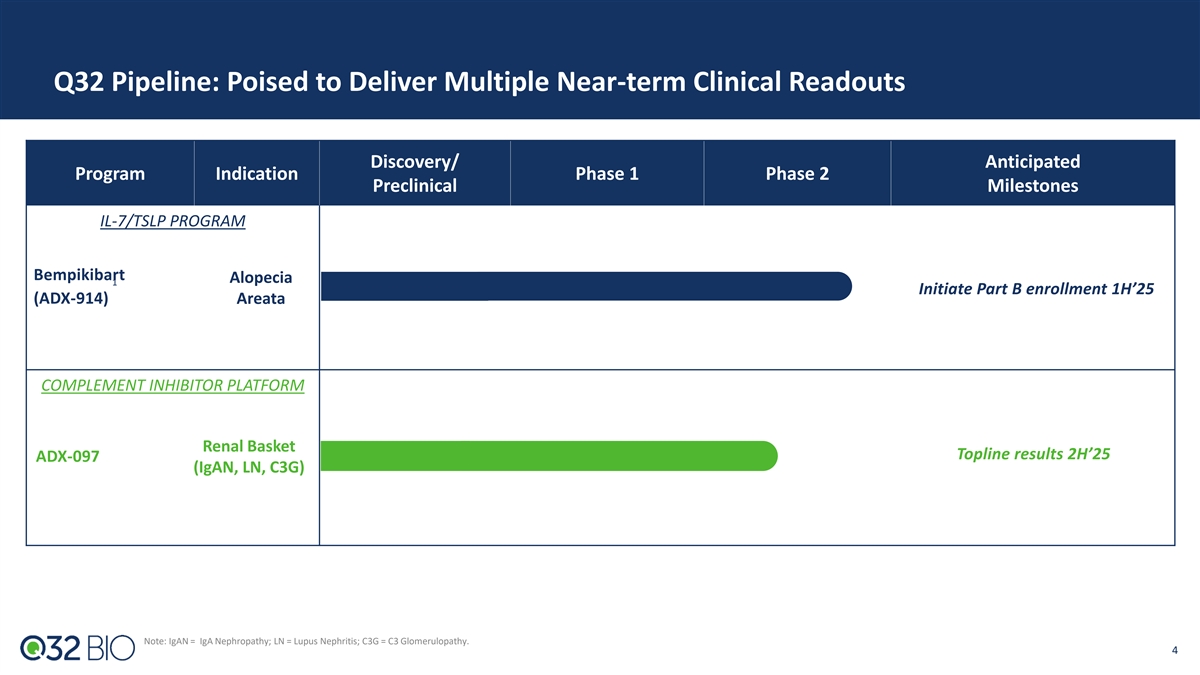
Q32 Pipeline: Poised to Deliver Multiple Near-term Clinical Readouts
Discovery/ Anticipated Program Indication Phase 1 Phase 2 Preclinical Milestones IL-7/TSLP PROGRAM Bempikibart Alopecia 1 Initiate Part B enrollment 1H’25 (ADX-914) Areata COMPLEMENT INHIBITOR PLATFORM Renal Basket Topline results 2H’25
ADX-097 (IgAN, LN, C3G) Note: IgAN = IgA Nephropathy; LN = Lupus Nephritis; C3G = C3 Glomerulopathy. 4
Bempikibart (ADX-914) (IL-7 / TSLP Receptor Inhibitor)
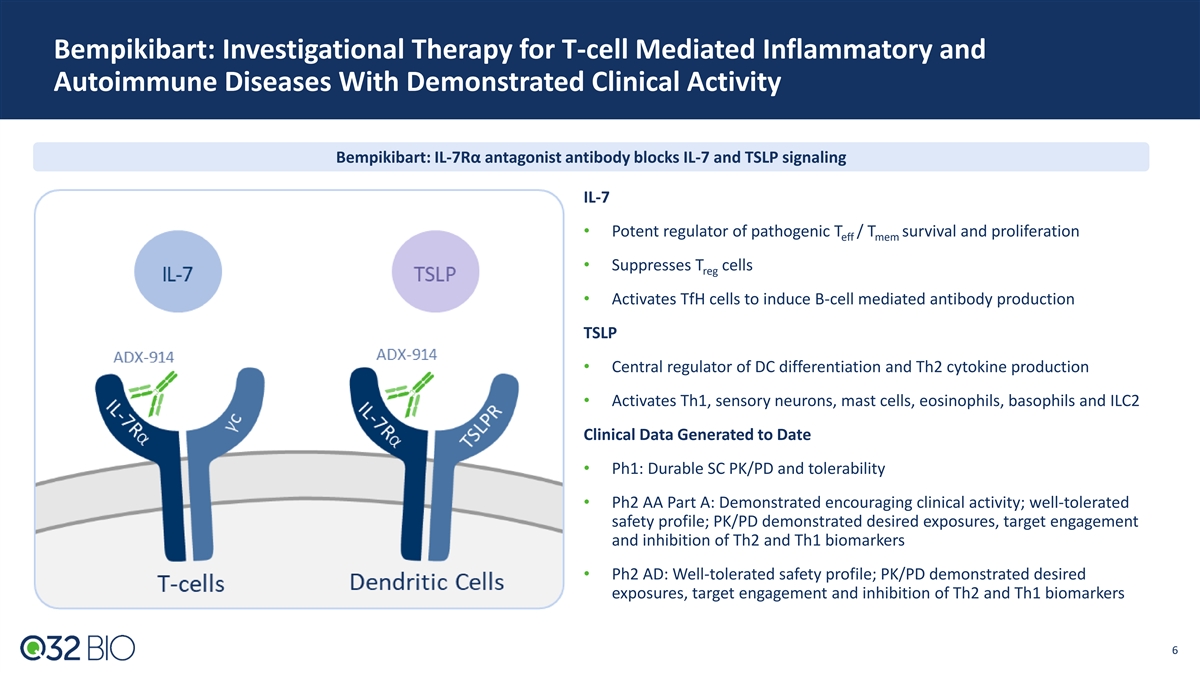
Bempikibart: Investigational Therapy for T-cell Mediated Inflammatory
and Autoimmune Diseases With Demonstrated Clinical Activity Bempikibart: IL-7Rα antagonist antibody blocks IL-7 and TSLP signaling IL-7 • Potent regulator of pathogenic T / T survival and proliferation eff mem • Suppresses T cells
reg • Activates TfH cells to induce B-cell mediated antibody production TSLP • Central regulator of DC differentiation and Th2 cytokine production • Activates Th1, sensory neurons, mast cells, eosinophils, basophils and ILC2
Clinical Data Generated to Date • Ph1: Durable SC PK/PD and tolerability • Ph2 AA Part A: Demonstrated encouraging clinical activity; well-tolerated safety profile; PK/PD demonstrated desired exposures, target engagement and inhibition
of Th2 and Th1 biomarkers • Ph2 AD: Well-tolerated safety profile; PK/PD demonstrated desired exposures, target engagement and inhibition of Th2 and Th1 biomarkers 6 6
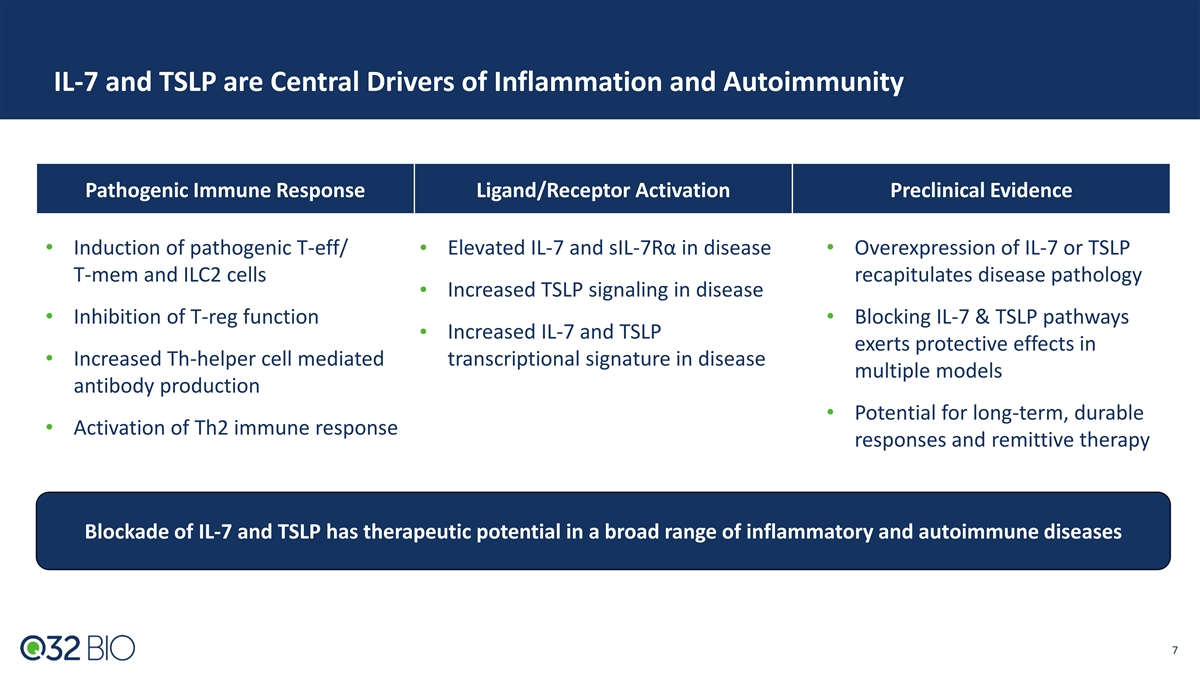
IL-7 and TSLP are Central Drivers of Inflammation and Autoimmunity
Pathogenic Immune Response Ligand/Receptor Activation Preclinical Evidence • Induction of pathogenic T-eff/ • Elevated IL-7 and sIL-7Rα in disease• Overexpression of IL-7 or TSLP T-mem and ILC2 cells recapitulates disease
pathology Increased TSLP signaling in disease • • Inhibition of T-reg function• Blocking IL-7 & TSLP pathways Increased IL-7 and TSLP • exerts protective effects in • Increased Th-helper cell mediated
transcriptional signature in disease multiple models antibody production • Potential for long-term, durable • Activation of Th2 immune response responses and remittive therapy Blockade of IL-7 and TSLP has therapeutic potential in a
broad range of inflammatory and autoimmune diseases 7
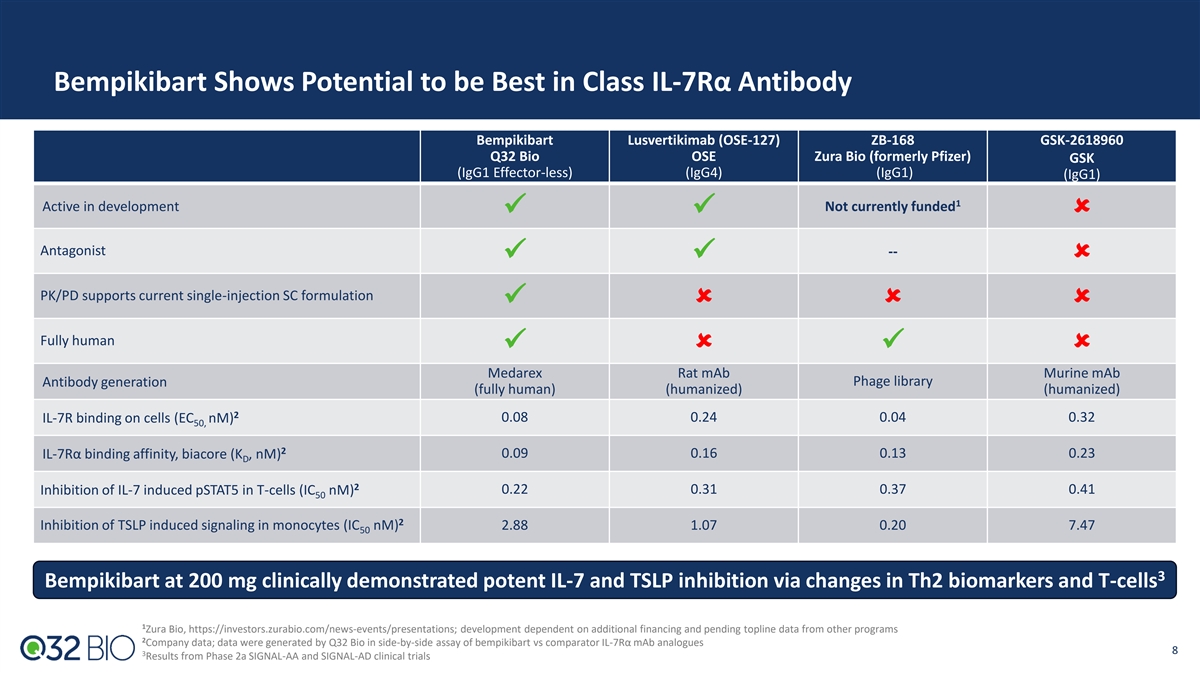
Bempikibart Shows Potential to be Best in Class IL-7Rα Antibody
Bempikibart Lusvertikimab (OSE-127) ZB-168 GSK-2618960 Q32 Bio OSE Zura Bio (formerly Pfizer) GSK (IgG1 Effector-less) (IgG4) (IgG1) (IgG1) 1 Active in development Not currently funded ✓✓û Antagonist -- ✓✓û
PK/PD supports current single-injection SC formulation ✓ûûû Fully human ✓û✓û Medarex Rat mAb Murine mAb Antibody generation Phage library (fully human) (humanized) (humanized) 2 IL-7R binding on cells
(EC nM) 0.08 0.24 0.04 0.32 50, 2 0.09 0.16 0.13 0.23 IL-7Rα binding affinity, biacore (K , nM) D 2 0.22 0.31 0.37 0.41 Inhibition of IL-7 induced pSTAT5 in T-cells (IC nM) 50 2 Inhibition of TSLP induced signaling in monocytes (IC nM) 2.88
1.07 0.20 7.47 50 3 Bempikibart at 200 mg clinically demonstrated potent IL-7 and TSLP inhibition via changes in Th2 biomarkers and T-cells 1 Zura Bio, https://investors.zurabio.com/news-events/presentations; development dependent on additional
financing and pending topline data from other programs 2 Company data; data were generated by Q32 Bio in side-by-side assay of bempikibart vs comparator IL-7Rα mAb analogues 8 3 Results from Phase 2a SIGNAL-AA and SIGNAL-AD clinical
trials
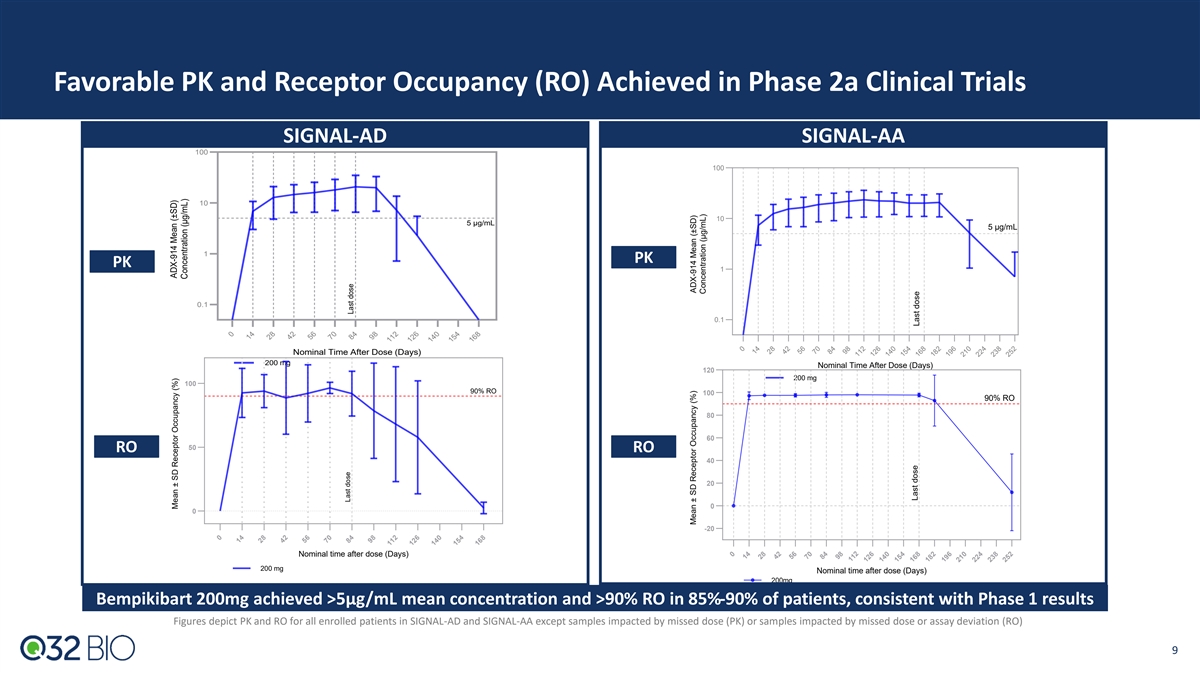
Favorable PK and Receptor Occupancy (RO) Achieved in Phase 2a Clinical
Trials SIGNAL-AD SIGNAL-AA 100 100 10 10 5 μg/mL 5 μg/mL 1 PK PK 1 0.1 0.1 Nominal Time After Dose (Days) 200 mg Nominal Time After Dose (Days) 120 200 mg 100 90% RO 100 90% RO 80 60 50 RO RO 40 20 0 0 -20 Nominal time after dose (Days)
200 mg Nominal time after dose (Days) 200mg Bempikibart 200mg achieved >5µg/mL mean concentration and >90% RO in 85%-90% of patients, consistent with Phase 1 results Figures depict PK and RO for all enrolled patients in SIGNAL-AD and
SIGNAL-AA except samples impacted by missed dose (PK) or samples impacted by missed dose or assay deviation (RO) 9 0 14 28 42 56 70 84 98 112 126 140 154 168 0 14 28 42 56 70 84 98 112 126 140 154 168 182 196 210 224 238 252 0 14 28 42 56 70 84 98
112 126 140 154 168 0 14 28 42 56 70 84 98 112 126 140 154 168 182 196 210 224 238 252 Mean ± SD Receptor Occupancy (%) ADX-914 Mean (±SD) Concentration (μg/mL) Last dose Last dose Mean ± SD Receptor Occupancy (%) ADX-914 Mean
(±SD) Concentration (μg/mL) Last dose Last dose
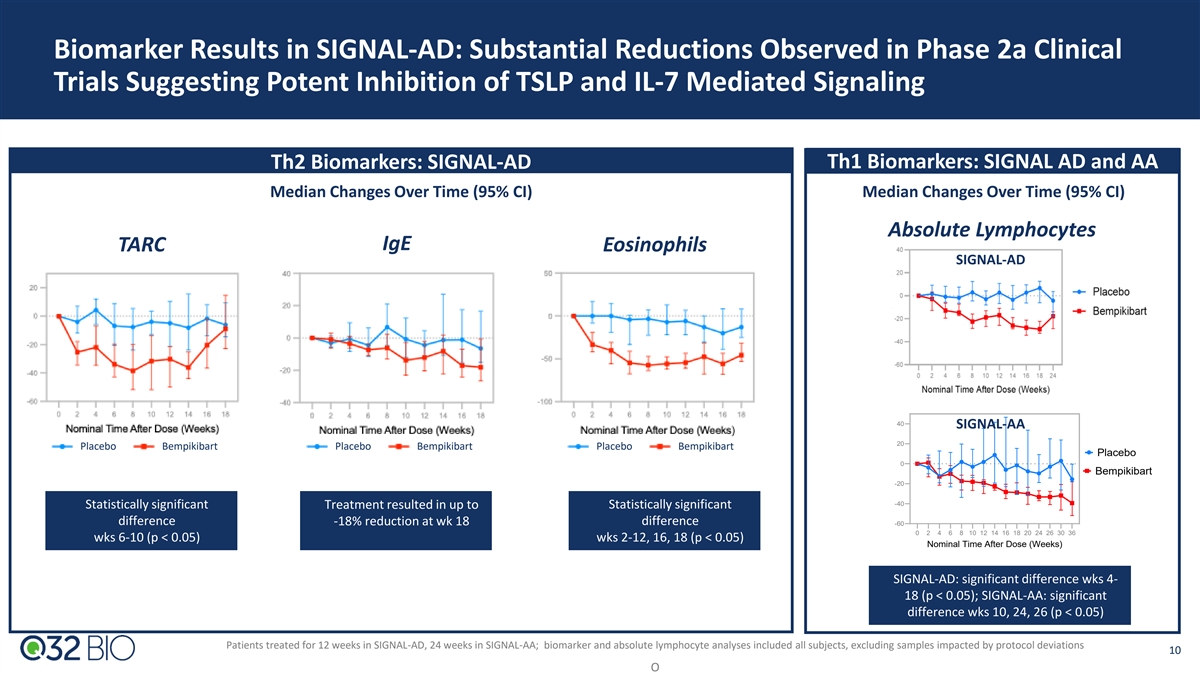
Biomarker Results in SIGNAL-AD: Substantial Reductions Observed in
Phase 2a Clinical Trials Suggesting Potent Inhibition of TSLP and IL-7 Mediated Signaling Th2 Biomarkers: SIGNAL-AD Th1 Biomarkers: SIGNAL AD and AA Median Changes Over Time (95% CI) Median Changes Over Time (95% CI) Absolute Lymphocytes IgE TARC
Eosinophils SIGNAL-AD 40 SIGNAL-AA 20 Placebo Bempikibart Placebo Bempikibart Placebo Bempikibart Placebo 0 Bempikibart -20 -40 Statistically significant Treatment resulted in up to Statistically significant difference -18% reduction at wk 18
difference -60 0 2 4 6 8 10 12 14 16 18 20 24 26 30 36 wks 6-10 (p < 0.05) wks 2-12, 16, 18 (p < 0.05) Nominal Time After Dose (Weeks) SIGNAL-AD: significant difference wks 4- 18 (p < 0.05); SIGNAL-AA: significant difference wks 10, 24, 26
(p < 0.05) Patients treated for 12 weeks in SIGNAL-AD, 24 weeks in SIGNAL-AA; biomarker and absolute lymphocyte analyses included all subjects, excluding samples impacted by protocol deviations 10 O % change from baseline Lymphocytes Median (95%
CI)
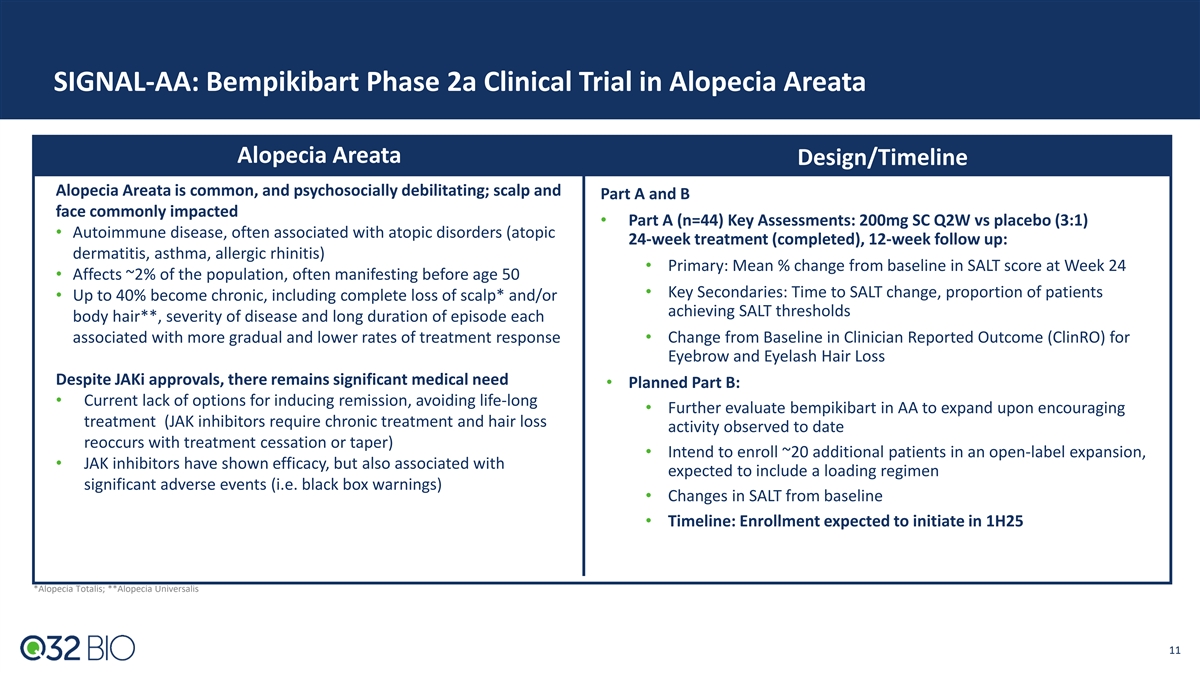
SIGNAL-AA: Bempikibart Phase 2a Clinical Trial in Alopecia Areata
Alopecia Areata Design/Timeline Alopecia Areata is common, and psychosocially debilitating; scalp and Part A and B face commonly impacted • Part A (n=44) Key Assessments: 200mg SC Q2W vs placebo (3:1) • Autoimmune disease, often
associated with atopic disorders (atopic 24-week treatment (completed), 12-week follow up: dermatitis, asthma, allergic rhinitis) • Primary: Mean % change from baseline in SALT score at Week 24 • Affects ~2% of the population, often
manifesting before age 50 • Key Secondaries: Time to SALT change, proportion of patients • Up to 40% become chronic, including complete loss of scalp* and/or achieving SALT thresholds body hair**, severity of disease and long duration of
episode each associated with more gradual and lower rates of treatment response• Change from Baseline in Clinician Reported Outcome (ClinRO) for Eyebrow and Eyelash Hair Loss Despite JAKi approvals, there remains significant medical need
• Planned Part B: • Current lack of options for inducing remission, avoiding life-long • Further evaluate bempikibart in AA to expand upon encouraging treatment (JAK inhibitors require chronic treatment and hair loss activity
observed to date reoccurs with treatment cessation or taper) • Intend to enroll ~20 additional patients in an open-label expansion, • JAK inhibitors have shown efficacy, but also associated with expected to include a loading regimen
significant adverse events (i.e. black box warnings) • Changes in SALT from baseline • Timeline: Enrollment expected to initiate in 1H25 *Alopecia Totalis; **Alopecia Universalis 11
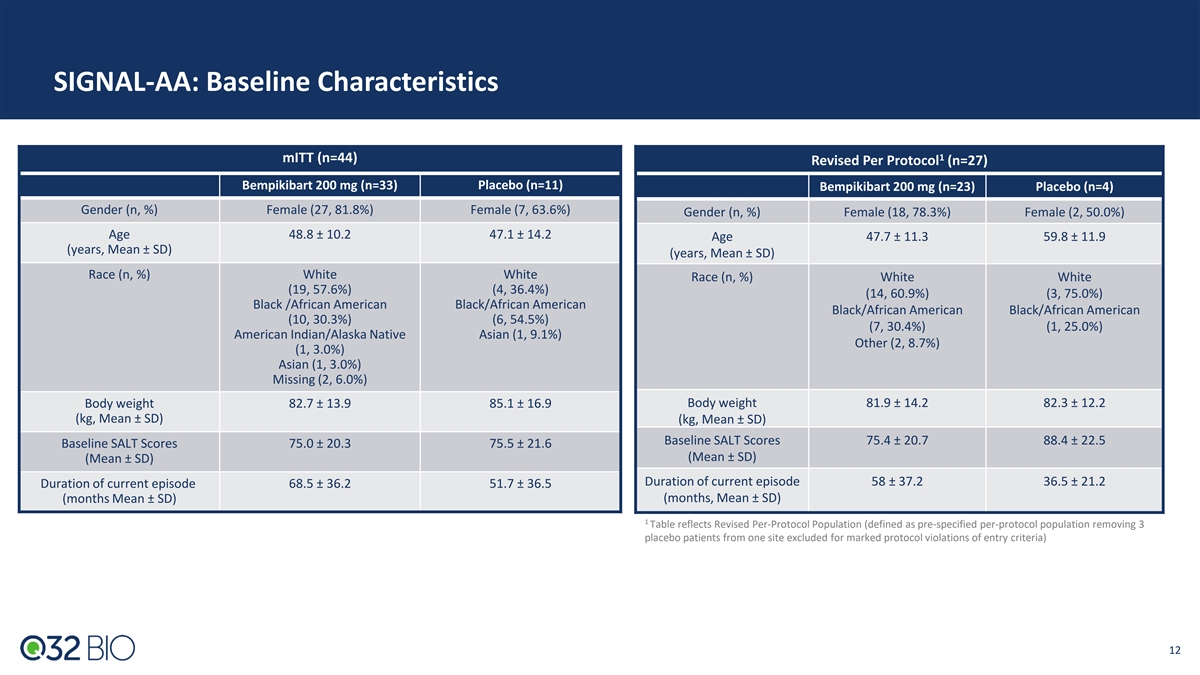
SIGNAL-AA: Baseline Characteristics 1 mITT (n=44) Revised Per Protocol
(n=27) Bempikibart 200 mg (n=33) Placebo (n=11) Bempikibart 200 mg (n=23) Placebo (n=4) Gender (n, %) Female (27, 81.8%) Female (7, 63.6%) Gender (n, %) Female (18, 78.3%) Female (2, 50.0%) Age 48.8 ± 10.2 47.1 ± 14.2 Age 47.7 ± 11.3
59.8 ± 11.9 (years, Mean ± SD) (years, Mean ± SD) Race (n, %) White White Race (n, %) White White (19, 57.6%) (4, 36.4%) (14, 60.9%) (3, 75.0%) Black /African American Black/African American Black/African American Black/African
American (10, 30.3%) (6, 54.5%) (7, 30.4%) (1, 25.0%) American Indian/Alaska Native Asian (1, 9.1%) Other (2, 8.7%) (1, 3.0%) Asian (1, 3.0%) Missing (2, 6.0%) Body weight 82.7 ± 13.9 85.1 ± 16.9 Body weight 81.9 ± 14.2 82.3 ±
12.2 (kg, Mean ± SD) (kg, Mean ± SD) Baseline SALT Scores 75.4 ± 20.7 88.4 ± 22.5 Baseline SALT Scores 75.0 ± 20.3 75.5 ± 21.6 (Mean ± SD) (Mean ± SD) Duration of current episode 58 ± 37.2 36.5 ±
21.2 Duration of current episode 68.5 ± 36.2 51.7 ± 36.5 (months Mean ± SD) (months, Mean ± SD) 1 Table reflects Revised Per-Protocol Population (defined as pre-specified per-protocol population removing 3 placebo patients from
one site excluded for marked protocol violations of entry criteria) 12 12
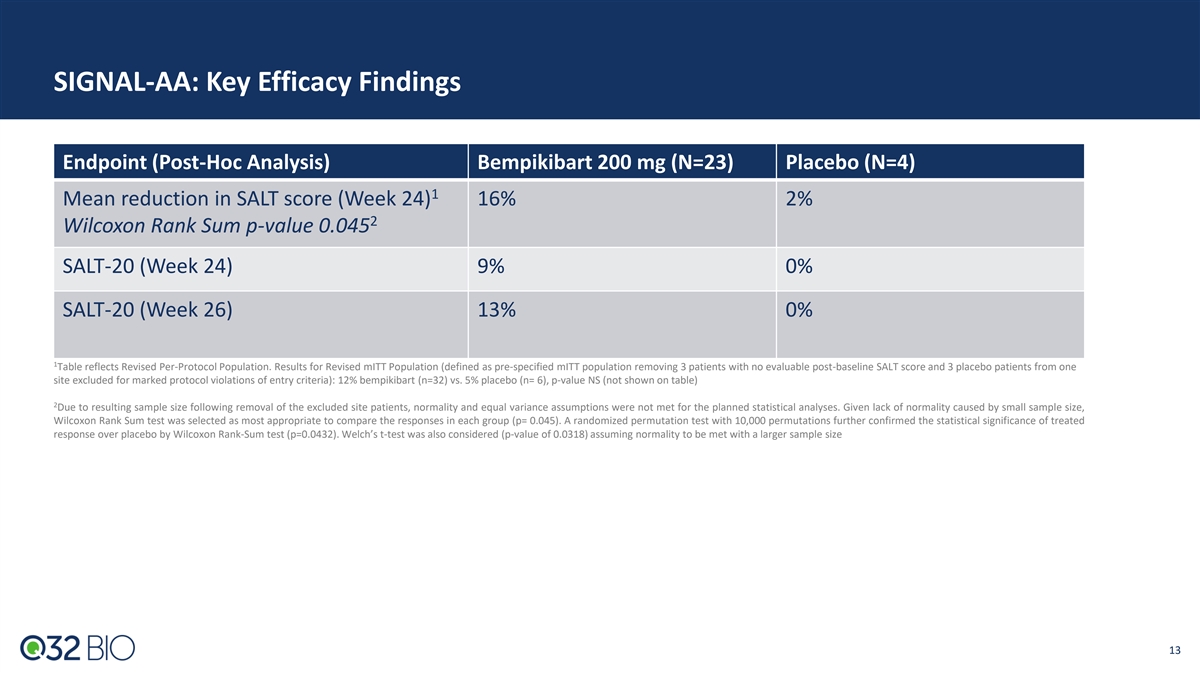
SIGNAL-AA: Key Efficacy Findings Endpoint (Post-Hoc Analysis)
Bempikibart 200 mg (N=23) Placebo (N=4) 1 Mean reduction in SALT score (Week 24) 16% 2% 2 Wilcoxon Rank Sum p-value 0.045 SALT-20 (Week 24) 9% 0% SALT-20 (Week 26) 13% 0% 1 Table reflects Revised Per-Protocol Population. Results for Revised mITT
Population (defined as pre-specified mITT population removing 3 patients with no evaluable post-baseline SALT score and 3 placebo patients from one site excluded for marked protocol violations of entry criteria): 12% bempikibart (n=32) vs. 5%
placebo (n= 6), p-value NS (not shown on table) 2 Due to resulting sample size following removal of the excluded site patients, normality and equal variance assumptions were not met for the planned statistical analyses. Given lack of normality
caused by small sample size, Wilcoxon Rank Sum test was selected as most appropriate to compare the responses in each group (p= 0.045). A randomized permutation test with 10,000 permutations further confirmed the statistical significance of treated
response over placebo by Wilcoxon Rank-Sum test (p=0.0432). Welch’s t-test was also considered (p-value of 0.0318) assuming normality to be met with a larger sample size 13 13
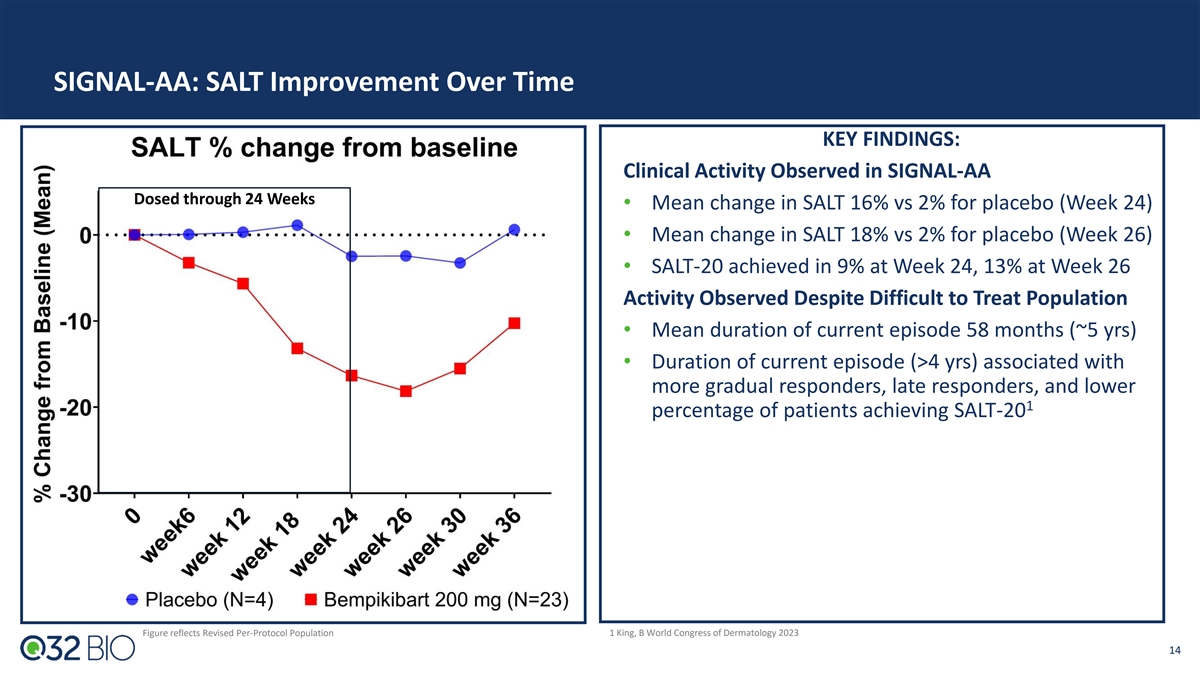
SIGNAL-AA: SALT Improvement Over Time KEY FINDINGS: Clinical Activity
Observed in SIGNAL-AA Dosed through 24 Weeks • Mean change in SALT 16% vs 2% for placebo (Week 24) • Mean change in SALT 18% vs 2% for placebo (Week 26) • SALT-20 achieved in 9% at Week 24, 13% at Week 26 Activity Observed Despite
Difficult to Treat Population • Mean duration of current episode 58 months (~5 yrs) • Duration of current episode (>4 yrs) associated with more gradual responders, late responders, and lower 1 percentage of patients achieving SALT-20
Figure reflects Revised Per-Protocol Population 1 King, B World Congress of Dermatology 2023 14
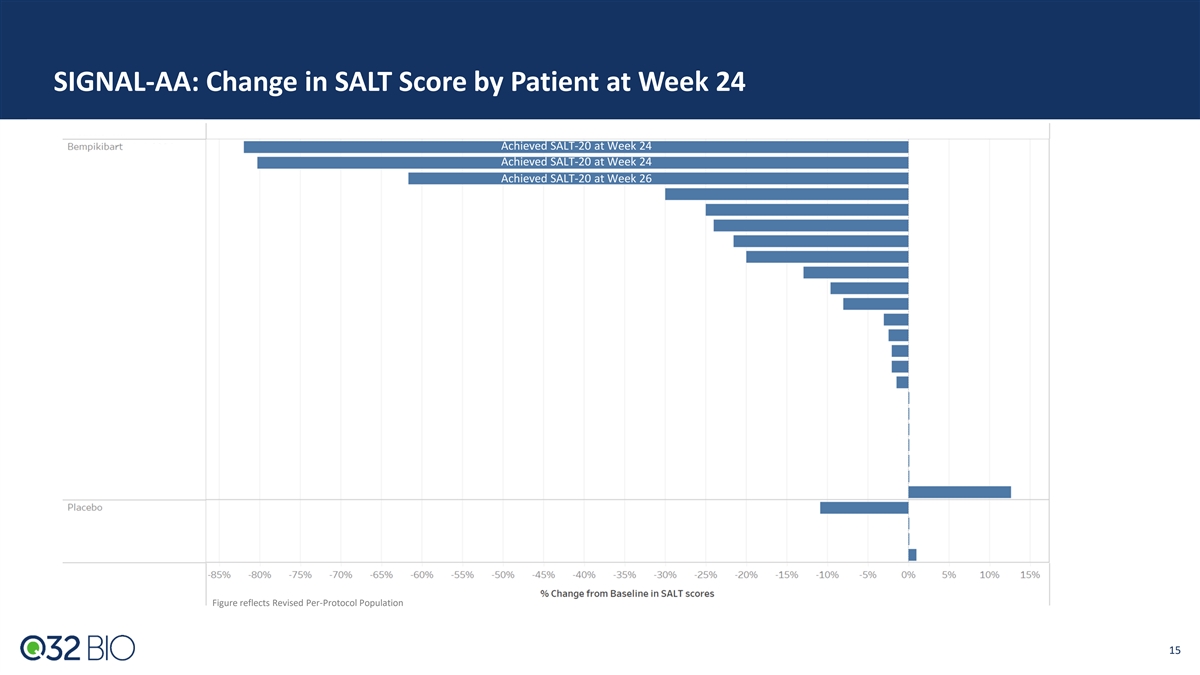
SIGNAL-AA: Change in SALT Score by Patient at Week 24 Achieved SALT-20
at Week 24 Achieved SALT-20 at Week 24 Achieved SALT-20 at Week 26 Figure reflects Revised Per-Protocol Population 15
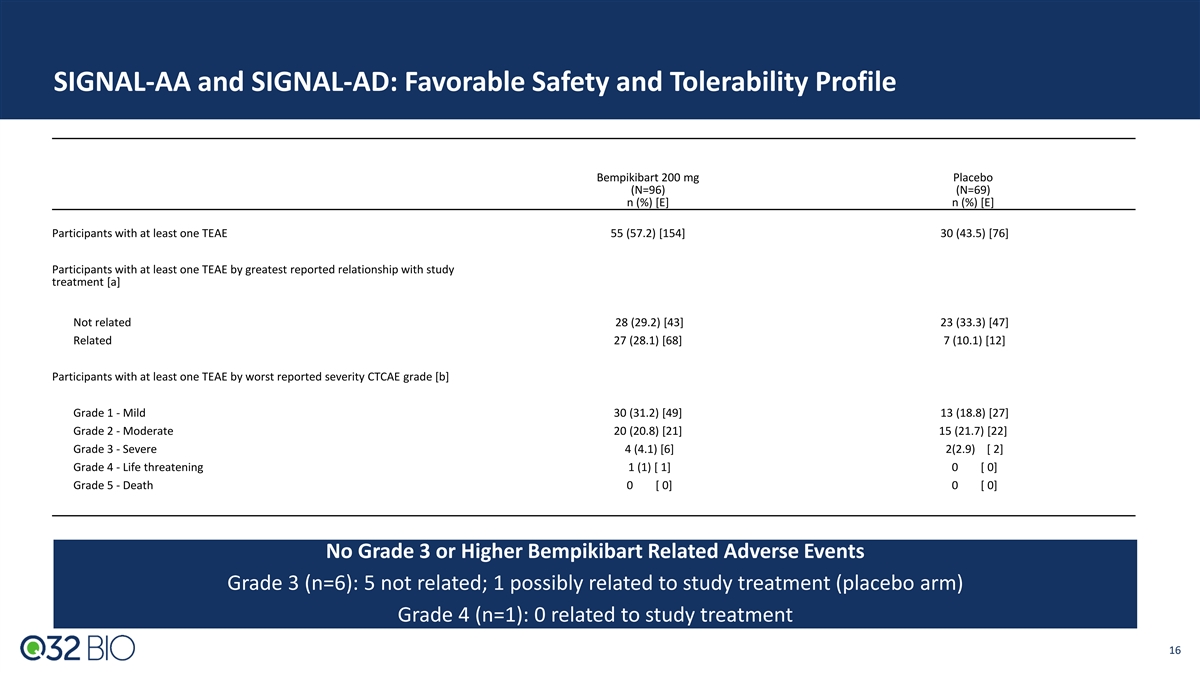
SIGNAL-AA and SIGNAL-AD: Favorable Safety and Tolerability Profile
Bempikibart 200 mg Placebo (N=96) (N=69) n (%) [E] n (%) [E] Participants with at least one TEAE 55 (57.2) [154] 30 (43.5) [76] Participants with at least one TEAE by greatest reported relationship with study treatment [a] Not related 28 (29.2) [43]
23 (33.3) [47] Related 27 (28.1) [68] 7 (10.1) [12] Participants with at least one TEAE by worst reported severity CTCAE grade [b] Grade 1 - Mild 30 (31.2) [49] 13 (18.8) [27] Grade 2 - Moderate 20 (20.8) [21] 15 (21.7) [22] Grade 3 - Severe 4 (4.1)
[6] 2(2.9) [ 2] Grade 4 - Life threatening 1 (1) [ 1] 0 [ 0] Grade 5 - Death 0 [ 0] 0 [ 0] No Grade 3 or Higher Bempikibart Related Adverse Events Grade 3 (n=6): 5 not related; 1 possibly related to study treatment (placebo arm) Grade 4 (n=1): 0
related to study treatment 16
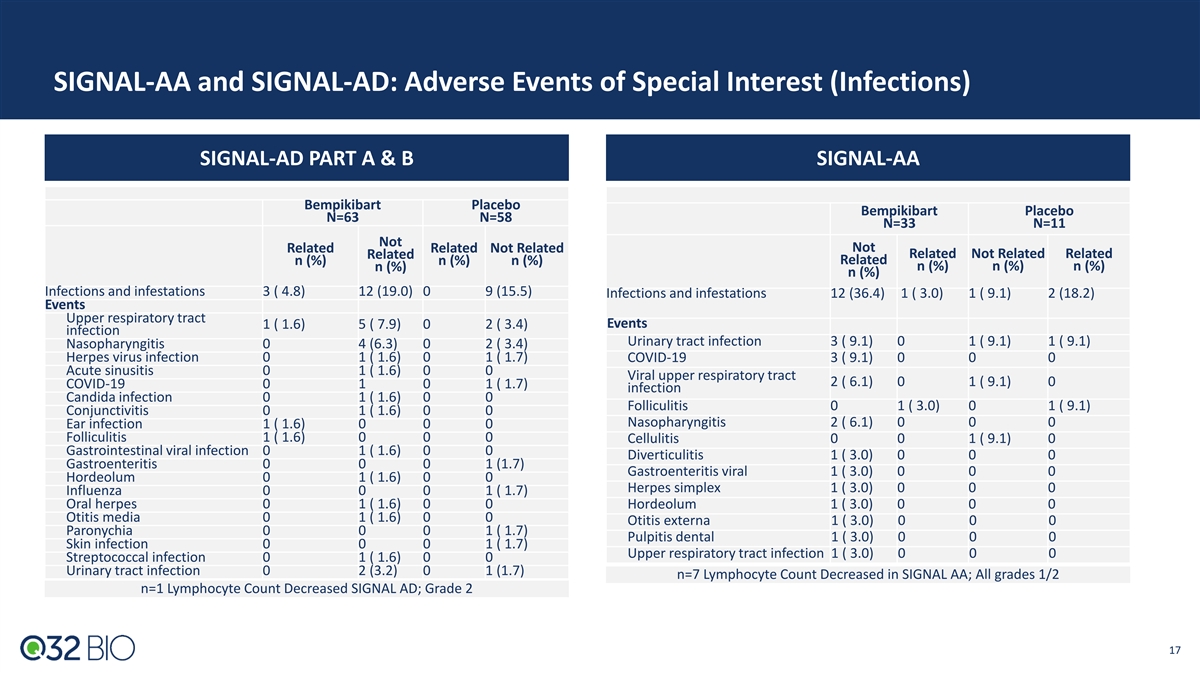
SIGNAL-AA and SIGNAL-AD: Adverse Events of Special Interest
(Infections) SIGNAL-AD PART A & B SIGNAL-AA Bempikibart Placebo Bempikibart Placebo N=63 N=58 N=33 N=11 Not Related Related Not Related Not Related Related Not Related Related n (%) n (%) n (%) Related n (%) n (%) n (%) n (%) n (%) Infections
and infestations 3 ( 4.8) 12 (19.0) 0 9 (15.5) Infections and infestations 12 (36.4) 1 ( 3.0) 1 ( 9.1) 2 (18.2) Events Upper respiratory tract Events 1 ( 1.6) 5 ( 7.9) 0 2 ( 3.4) infection Urinary tract infection 3 ( 9.1) 0 1 ( 9.1) 1 ( 9.1)
Nasopharyngitis 0 4 (6.3) 0 2 ( 3.4) Herpes virus infection 0 1 ( 1.6) 0 1 ( 1.7) COVID-19 3 ( 9.1) 0 0 0 Acute sinusitis 0 1 ( 1.6) 0 0 Viral upper respiratory tract 2 ( 6.1) 0 1 ( 9.1) 0 COVID-19 0 1 0 1 ( 1.7) infection Candida infection 0 1 (
1.6) 0 0 Folliculitis 0 1 ( 3.0) 0 1 ( 9.1) Conjunctivitis 0 1 ( 1.6) 0 0 Nasopharyngitis 2 ( 6.1) 0 0 0 Ear infection 1 ( 1.6) 0 0 0 Folliculitis 1 ( 1.6) 0 0 0 Cellulitis 0 0 1 ( 9.1) 0 Gastrointestinal viral infection 0 1 ( 1.6) 0 0
Diverticulitis 1 ( 3.0) 0 0 0 Gastroenteritis 0 0 0 1 (1.7) Gastroenteritis viral 1 ( 3.0) 0 0 0 Hordeolum 0 1 ( 1.6) 0 0 Herpes simplex 1 ( 3.0) 0 0 0 Influenza 0 0 0 1 ( 1.7) Oral herpes 0 1 ( 1.6) 0 0 Hordeolum 1 ( 3.0) 0 0 0 Otitis media 0 1 (
1.6) 0 0 Otitis externa 1 ( 3.0) 0 0 0 Paronychia 0 0 0 1 ( 1.7) Pulpitis dental 1 ( 3.0) 0 0 0 Skin infection 0 0 0 1 ( 1.7) Upper respiratory tract infection 1 ( 3.0) 0 0 0 Streptococcal infection 0 1 ( 1.6) 0 0 Urinary tract infection 0 2 (3.2) 0
1 (1.7) n=7 Lymphocyte Count Decreased in SIGNAL AA; All grades 1/2 n=1 Lymphocyte Count Decreased SIGNAL AD; Grade 2 17
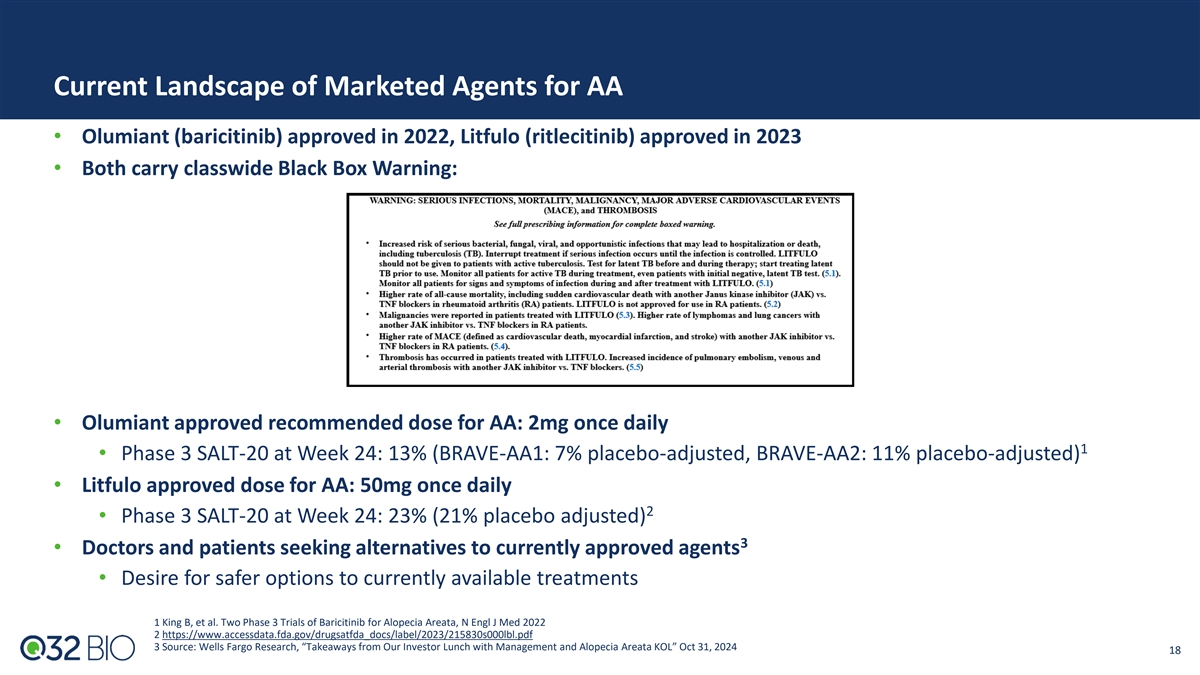
Current Landscape of Marketed Agents for AA • Olumiant
(baricitinib) approved in 2022, Litfulo (ritlecitinib) approved in 2023 • Both carry classwide Black Box Warning: • Olumiant approved recommended dose for AA: 2mg once daily 1 • Phase 3 SALT-20 at Week 24: 13% (BRAVE-AA1: 7%
placebo-adjusted, BRAVE-AA2: 11% placebo-adjusted) • Litfulo approved dose for AA: 50mg once daily 2 • Phase 3 SALT-20 at Week 24: 23% (21% placebo adjusted) 3 • Doctors and patients seeking alternatives to currently approved
agents • Desire for safer options to currently available treatments 1 King B, et al. Two Phase 3 Trials of Baricitinib for Alopecia Areata, N Engl J Med 2022 2 https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215830s000lbl.pdf 3
Source: Wells Fargo Research, “Takeaways from Our Investor Lunch with Management and Alopecia Areata KOL” Oct 31, 2024 18

Tissue Targeted Platform: Building The Future of Complement
Therapeutics
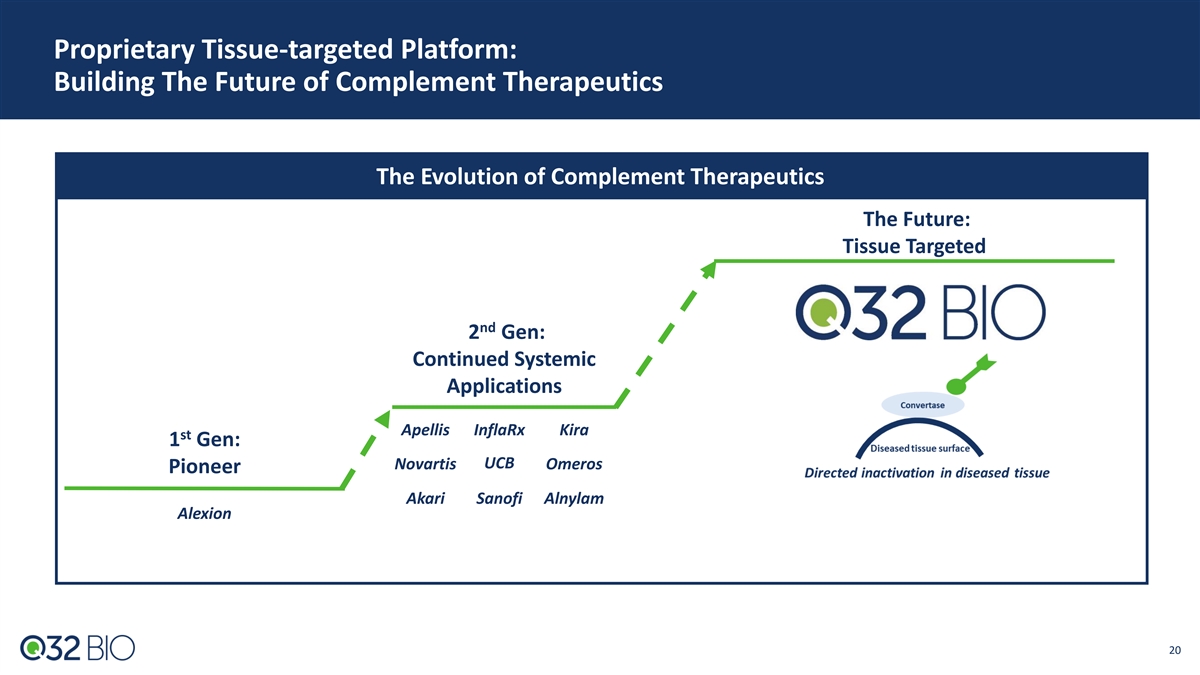
Proprietary Tissue-targeted Platform: Building The Future of Complement
Therapeutics The Evolution of Complement Therapeutics The Future: Tissue Targeted nd 2 Gen: Continued Systemic Applications Apellis InflaRx Kira st 1 Gen: UCB Novartis Omeros Pioneer Akari Sanofi Alnylam Alexion 20
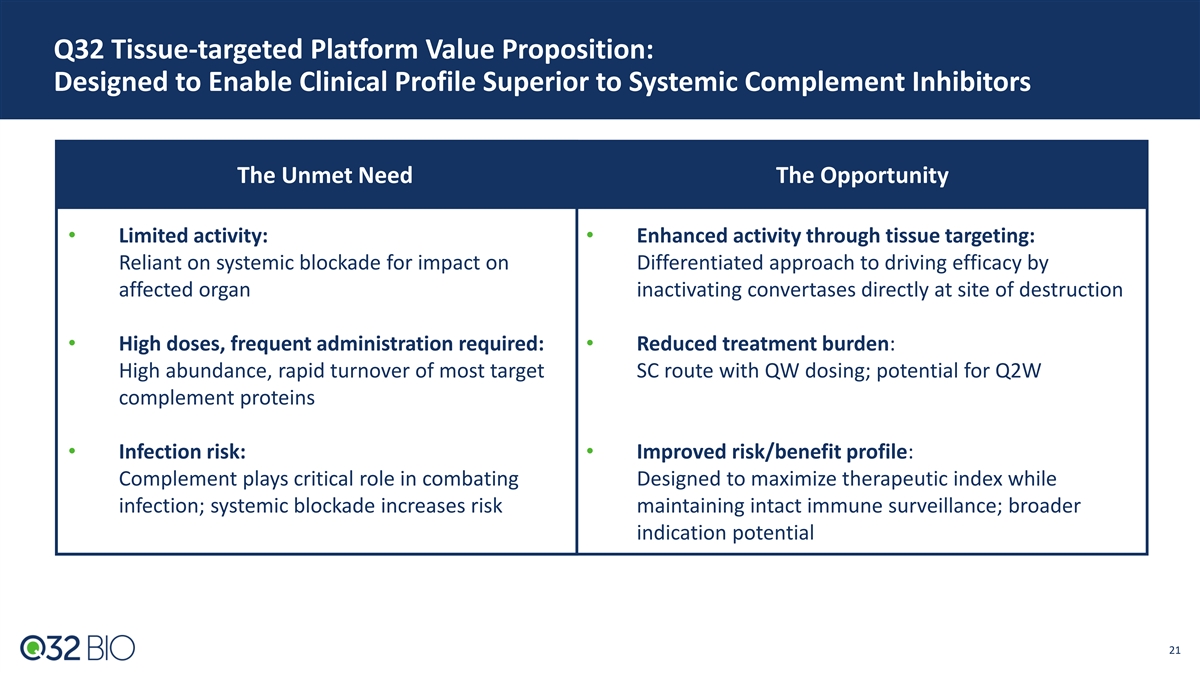
Q32 Tissue-targeted Platform Value Proposition: Designed to Enable
Clinical Profile Superior to Systemic Complement Inhibitors The Unmet Need The Opportunity • Limited activity: • Enhanced activity through tissue targeting: Reliant on systemic blockade for impact on Differentiated approach to driving
efficacy by affected organ inactivating convertases directly at site of destruction • High doses, frequent administration required: • R ed u ced tr e a tme nt burden: High abundance, rapid turnover of most target SC route with QW dosing;
potential for Q2W complement proteins • Infection risk: • Improved risk/benefit profile: Complement plays critical role in combating Designed to maximize therapeutic index while infection; systemic blockade increases risk maintaining
intact immune surveillance; broader indication potential 21
ADX-097 (C3d targeted antibody – fH 1-5 fusion protein)
ADX-097: A Novel Tissue-Targeted Approach to Regulating the Complement
System ADX-097 Design: C3d antibody – fH 1-5 ADX-097 Construct: humanized anti-C3d mAb linked to two moieties of a negative regulatory protein (fH ) 1-5 • Designed to be active at the site of complement activation in the tissue without
systemic impact • Inactivation of alternative pathway convertases gains control of amplification loop and all 3 complement pathways Clinical Data Completed to Date: • Ph1 completed: supported dose selection and continued advancement
• 450mg SC QW selected: Ph1 confirmed SC dosing (with possibility to further reduce frequency), demonstrated exposures above predicted range for clinical activity, while below systemic inhibition Topline Data Expected 2H’25 • Renal
basket Ph2 topline data (initial data 1H’25) 23 23
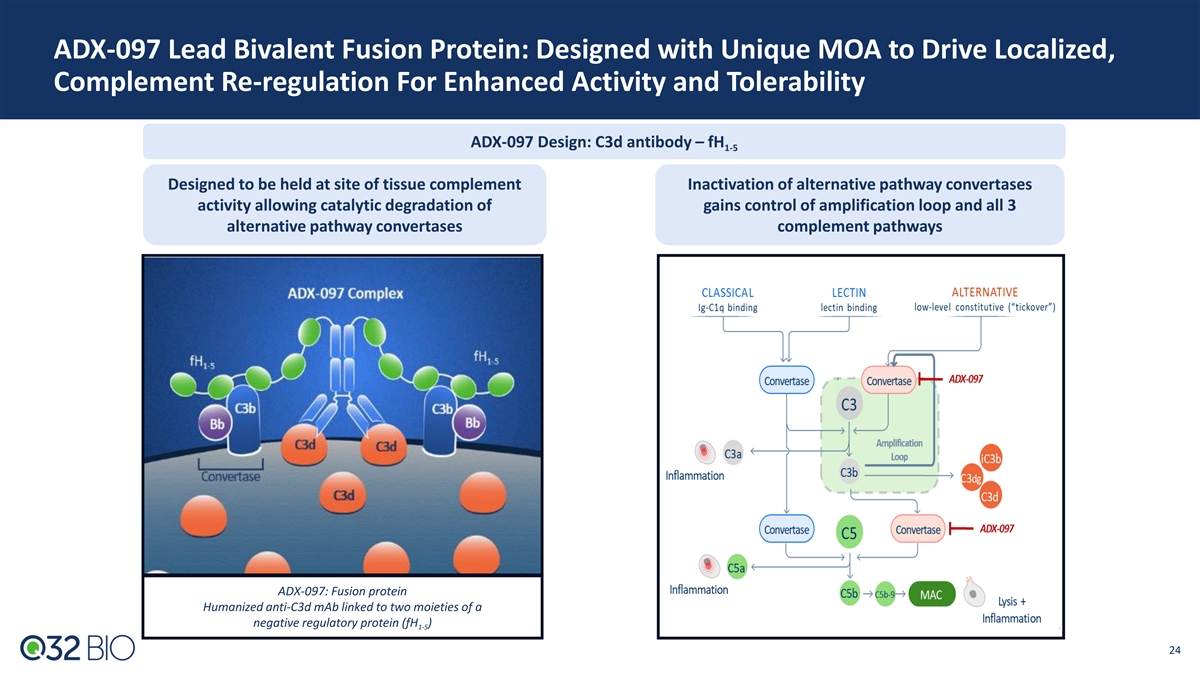
ADX-097 Lead Bivalent Fusion Protein: Designed with Unique MOA to Drive
Localized, Complement Re-regulation For Enhanced Activity and Tolerability ADX-097 Design: C3d antibody – fH 1-5 Designed to be held at site of tissue complement Inactivation of alternative pathway convertases activity allowing catalytic
degradation of gains control of amplification loop and all 3 alternative pathway convertases complement pathways ADX-097: Fusion protein Humanized anti-C3d mAb linked to two moieties of a negative regulatory protein (fH ) 1-5 24 24
ADX-097 Preclinical and Ph1 Data: Robust Data Package Supports Desired
PK and PD with Favorable Tolerability and Immunogenicity Profile Preclinical Data • Tissue distribution and target binding • Durable (>7 days) tissue PK/PD after SC dosing • Reduction in key proof of mechanism (POM)/proof of
concept (POC) biomarkers including proteinuria and albuminuria • >40X safety margin for planned Ph2 clinical dosing Ph1 Clinical Data • Favorable tolerability and good immunogenicity profile across all SAD/MAD doses • Weekly SC
dosing met desired exposures for predicted complete tissue inhibition (based on preclinical modeling) with no systemic inhibition • Proximal POM supports in-vivo ADX-097 integrity 25 25
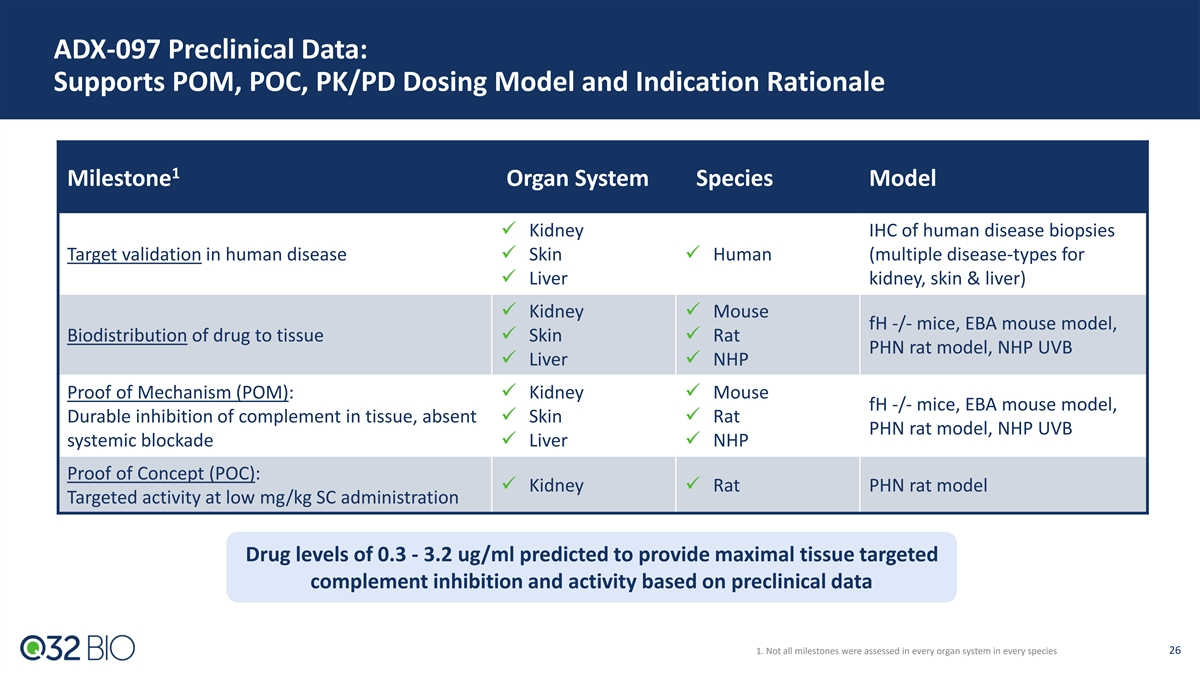
ADX-097 Preclinical Data: Supports POM, POC, PK/PD Dosing Model and
Indication Rationale 1 Milestone Organ System Species Model ✓ Kidney IHC of human disease biopsies Target validation in human disease✓ Skin✓ Human (multiple disease-types for ✓ Liver kidney, skin & liver) ✓
Kidney✓ Mouse fH -/- mice, EBA mouse model, Biodistribution of drug to tissue✓ Skin✓ Rat PHN rat model, NHP UVB ✓ Liver✓ NHP Proof of Mechanism (POM): ✓ Kidney✓ Mouse fH -/- mice, EBA mouse model,
Durable inhibition of complement in tissue, absent ✓ Skin✓ Rat PHN rat model, NHP UVB systemic blockade✓ Liver✓ NHP Proof of Concept (POC): ✓ Kidney✓ Rat PHN rat model Targeted activity at low mg/kg SC
administration Drug levels of 0.3 - 3.2 ug/ml predicted to provide maximal tissue targeted complement inhibition and activity based on preclinical data 1. Not all milestones were assessed in every organ system in every species 26
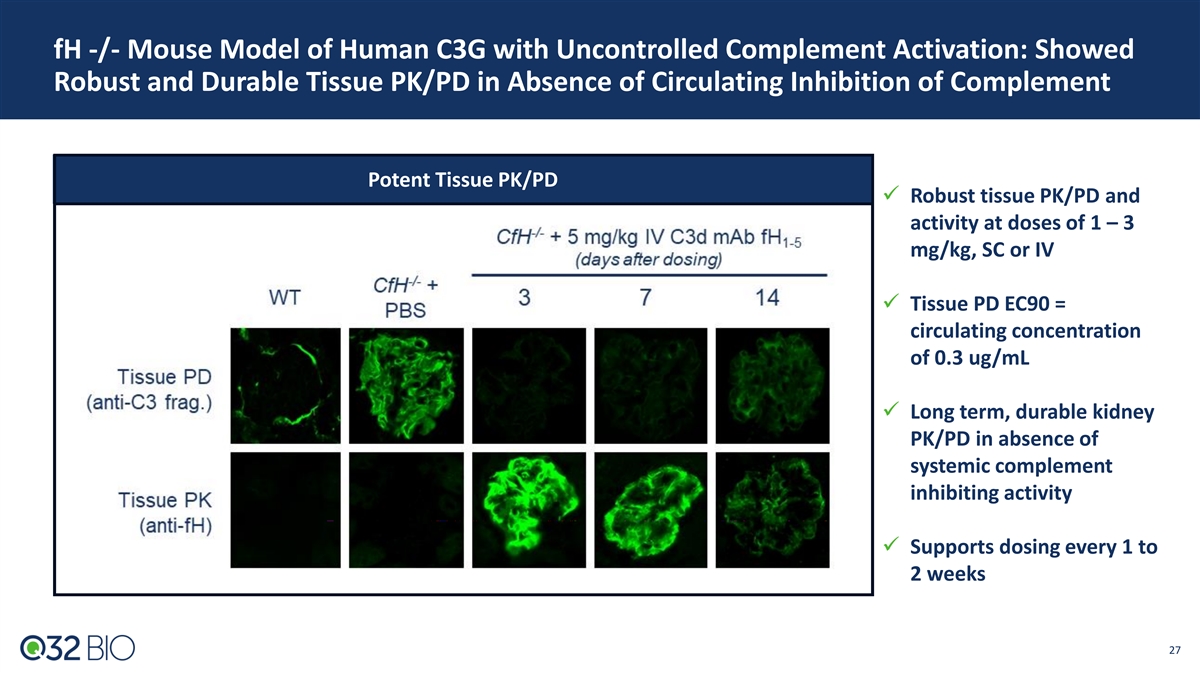
fH -/- Mouse Model of Human C3G with Uncontrolled Complement
Activation: Showed Robust and Durable Tissue PK/PD in Absence of Circulating Inhibition of Complement Potent Tissue PK/PD ✓ Robust tissue PK/PD and activity at doses of 1 – 3 mg/kg, SC or IV ✓ Tissue PD EC90 = circulating
concentration of 0.3 ug/mL ✓ Long term, durable kidney PK/PD in absence of systemic complement inhibiting activity ✓ Supports dosing every 1 to 2 weeks 27
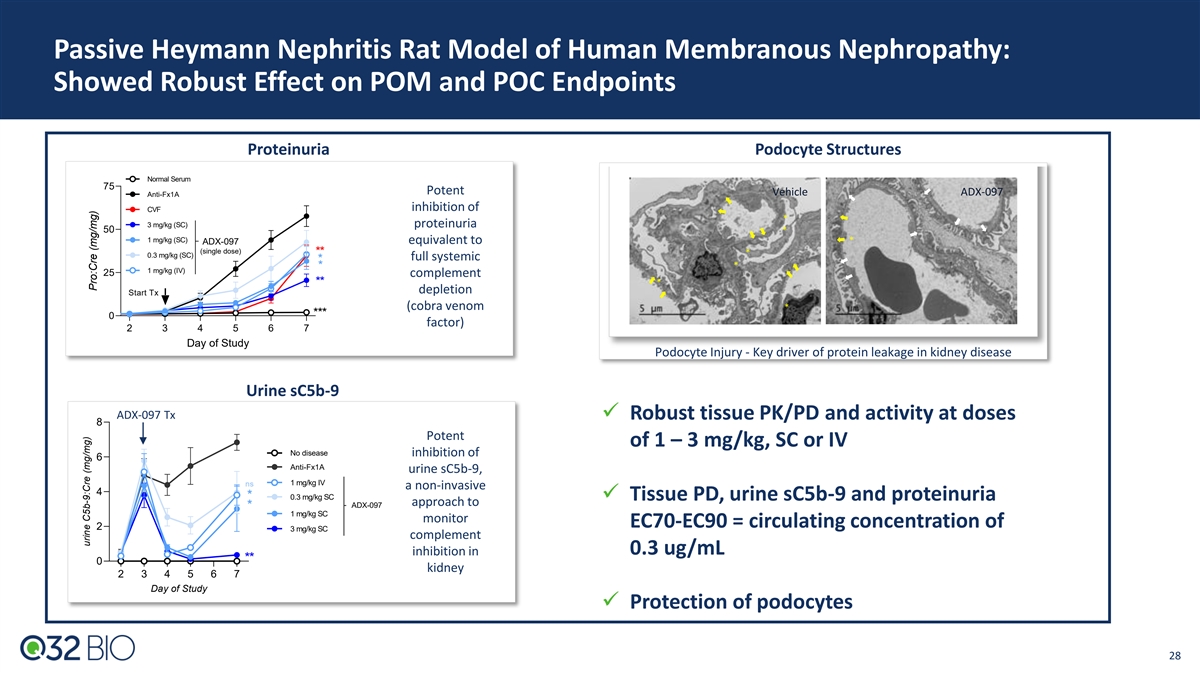
Passive Heymann Nephritis Rat Model of Human Membranous Nephropathy:
Showed Robust Effect on POM and POC Endpoints Proteinuria Podocyte Structures Normal Serum 75 Potent Vehicle ADX-097 Anti-Fx1A inhibition of CVF * 3 mg/kg (SC) proteinuria 50 * 1 mg/kg (SC) equivalent to * ADX-097 (single dose) ** * 0.3 mg/kg (SC)
full systemic * * * 1 mg/kg (IV) 25 complement * ** depletion Start Tx (cobra venom * *** 0 factor) 2 3 4 5 6 7 Day of Study Podocyte Injury - Key driver of protein leakage in kidney disease Urine sC5b-9 ADX-097 Tx ✓ Robust tissue PK/PD and
activity at doses 8 Potent of 1 – 3 mg/kg, SC or IV No disease inhibition of 6 Anti-Fx1A urine sC5b-9, 1 mg/kg IV ns a non-invasive 4 * 0.3 mg/kg SC ✓ Tissue PD, urine sC5b-9 and proteinuria approach to ADX-097 * 1 mg/kg SC monitor
EC70-EC90 = circulating concentration of 2 3 mg/kg SC complement inhibition in 0.3 ug/mL ** 0 kidney 2 3 4 5 6 7 Day of Study ✓ Protection of podocytes 28 urine C5b-9:Cre (mg/mg) Pro:Cre (mg/mg)
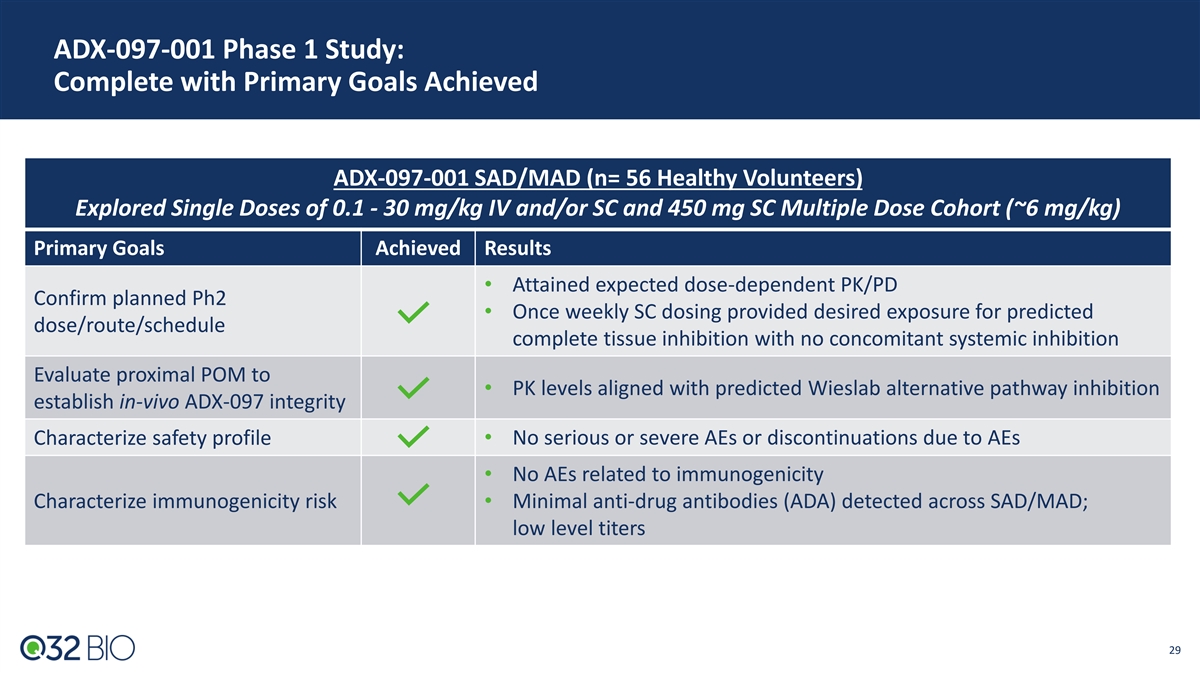
ADX-097-001 Phase 1 Study: Complete with Primary Goals Achieved
ADX-097-001 SAD/MAD (n= 56 Healthy Volunteers) Explored Single Doses of 0.1 - 30 mg/kg IV and/or SC and 450 mg SC Multiple Dose Cohort (~6 mg/kg) Primary Goals Achieved Results • Attained expected dose-dependent PK/PD Confirm planned Ph2
• Once weekly SC dosing provided desired exposure for predicted dose/route/schedule complete tissue inhibition with no concomitant systemic inhibition Evaluate proximal POM to • PK levels aligned with predicted Wieslab alternative
pathway inhibition establish in-vivo ADX-097 integrity Characterize safety profile• No serious or severe AEs or discontinuations due to AEs • No AEs related to immunogenicity Characterize immunogenicity risk• Minimal anti-drug
antibodies (ADA) detected across SAD/MAD; low level titers 29
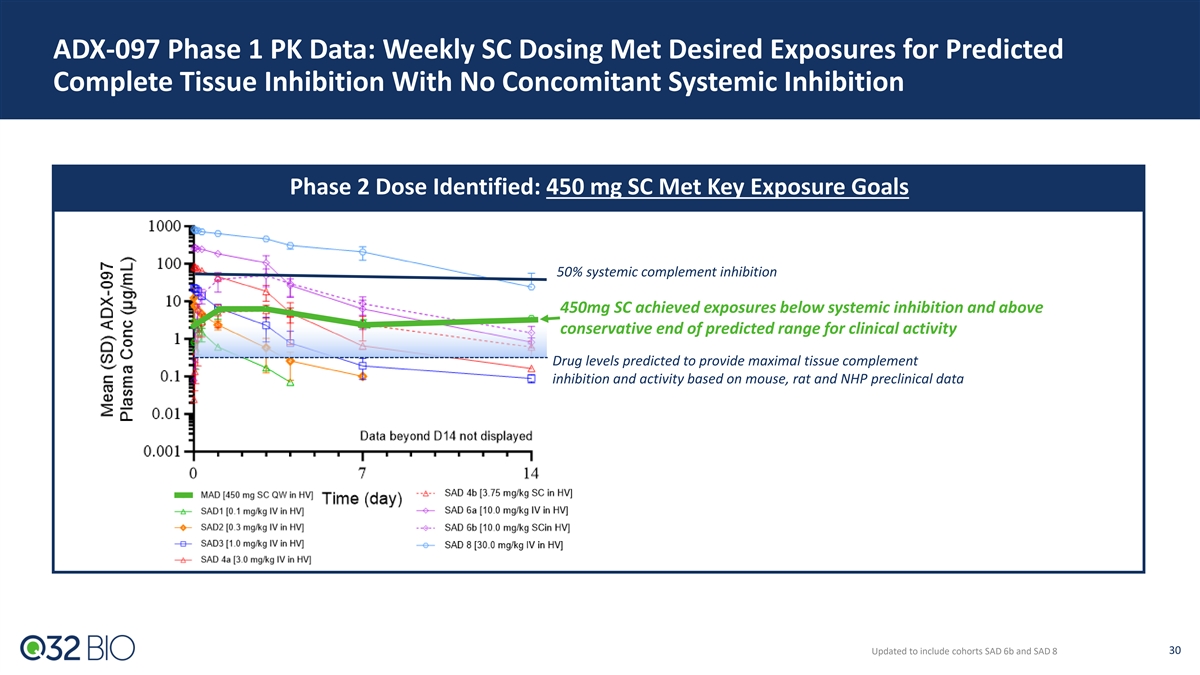
ADX-097 Phase 1 PK Data: Weekly SC Dosing Met Desired Exposures for
Predicted Complete Tissue Inhibition With No Concomitant Systemic Inhibition Phase 2 Dose Identified: 450 mg SC Met Key Exposure Goals 50% systemic complement inhibition 450mg SC achieved exposures below systemic inhibition and above conservative
end of predicted range for clinical activity Drug levels predicted to provide maximal tissue complement inhibition and activity based on mouse, rat and NHP preclinical data 30 Updated to include cohorts SAD 6b and SAD 8
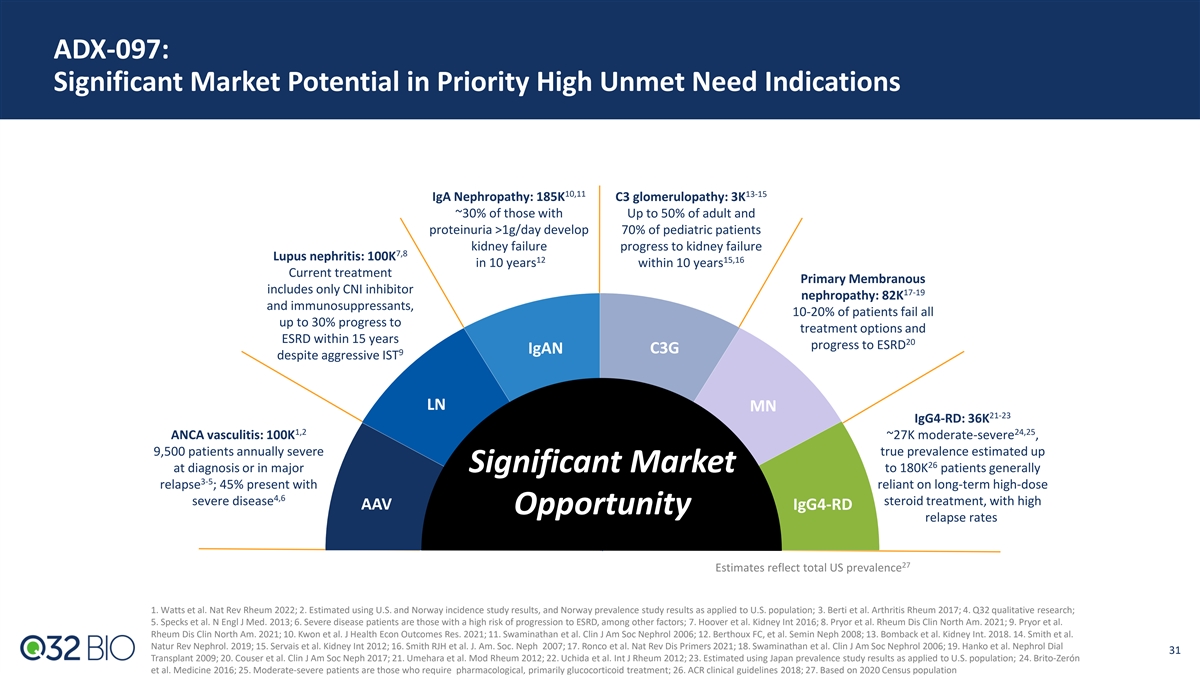
ADX-097: Significant Market Potential in Priority High Unmet Need
Indications 10,11 13-15 IgA Nephropathy: 185K C3 glomerulopathy: 3K ~30% of those with Up to 50% of adult and proteinuria >1g/day develop 70% of pediatric patients kidney failure progress to kidney failure 7,8 Lupus nephritis: 100K 12 15,16 in 10
years within 10 years Current treatment Primary Membranous includes only CNI inhibitor 17-19 nephropathy: 82K and immunosuppressants, 10-20% of patients fail all up to 30% progress to treatment options and ESRD within 15 years 20 progress to ESRD
IgAN C3G 9 despite aggressive IST LN MN 21-23 IgG4-RD: 36K 1,2 24,25 ANCA vasculitis: 100K ~27K moderate-severe , 9,500 patients annually severe true prevalence estimated up 26 at diagnosis or in major Significant Market to 180K patients generally
3-5 relapse ; 45% present with reliant on long-term high-dose 4,6 severe disease steroid treatment, with high AAV IgG4-RD Opportunity relapse rates 27 Estimates reflect total US prevalence 1. Watts et al. Nat Rev Rheum 2022; 2. Estimated using U.S.
and Norway incidence study results, and Norway prevalence study results as applied to U.S. population; 3. Berti et al. Arthritis Rheum 2017; 4. Q32 qualitative research; 5. Specks et al. N Engl J Med. 2013; 6. Severe disease patients are those with
a high risk of progression to ESRD, among other factors; 7. Hoover et al. Kidney Int 2016; 8. Pryor et al. Rheum Dis Clin North Am. 2021; 9. Pryor et al. Rheum Dis Clin North Am. 2021; 10. Kwon et al. J Health Econ Outcomes Res. 2021; 11.
Swaminathan et al. Clin J Am Soc Nephrol 2006; 12. Berthoux FC, et al. Semin Neph 2008; 13. Bomback et al. Kidney Int. 2018. 14. Smith et al. Natur Rev Nephrol. 2019; 15. Servais et al. Kidney Int 2012; 16. Smith RJH et al. J. Am. Soc. Neph 2007;
17. Ronco et al. Nat Rev Dis Primers 2021; 18. Swaminathan et al. Clin J Am Soc Nephrol 2006; 19. Hanko et al. Nephrol Dial 31 Transplant 2009; 20. Couser et al. Clin J Am Soc Neph 2017; 21. Umehara et al. Mod Rheum 2012; 22. Uchida et al. Int J
Rheum 2012; 23. Estimated using Japan prevalence study results as applied to U.S. population; 24. Brito-Zerón et al. Medicine 2016; 25. Moderate-severe patients are those who require pharmacological, primarily glucocorticoid treatment; 26. ACR
clinical guidelines 2018; 27. Based on 2020 Census population
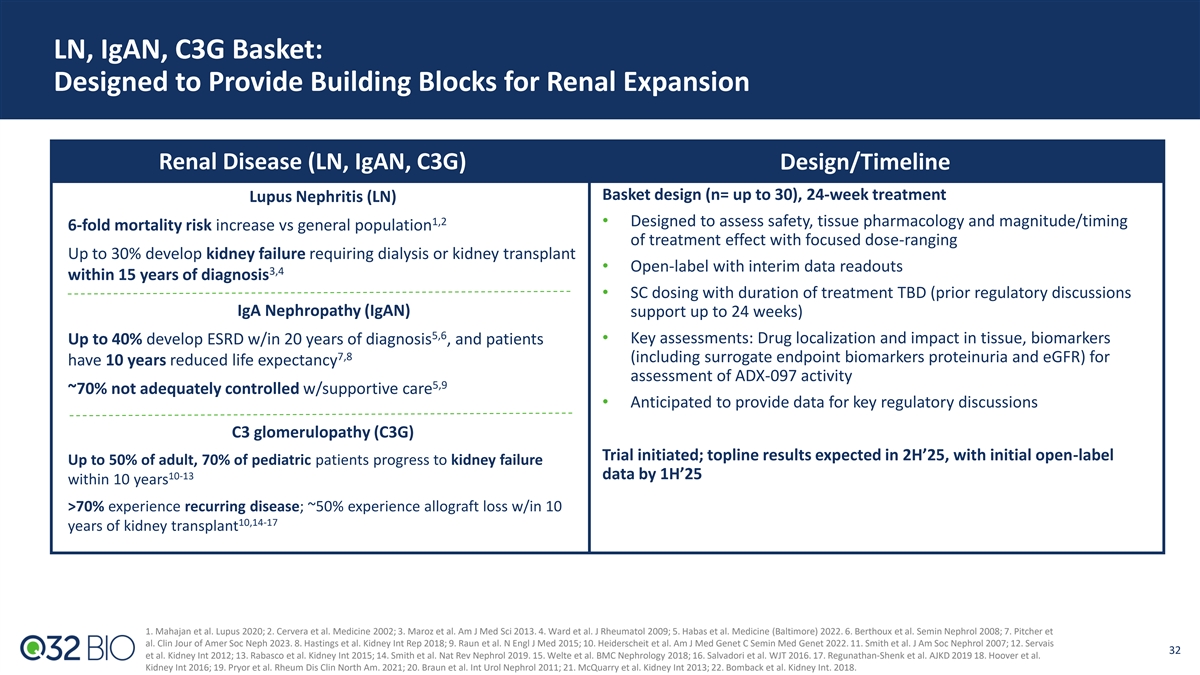
LN, IgAN, C3G Basket: Designed to Provide Building Blocks for Renal
Expansion Renal Disease (LN, IgAN, C3G) Design/Timeline Basket design (n= up to 30), 24-week treatment Lupus Nephritis (LN) 1,2 • Designed to assess safety, tissue pharmacology and magnitude/timing 6-fold mortality risk increase vs general
population of treatment effect with focused dose-ranging Up to 30% develop kidney failure requiring dialysis or kidney transplant • Open-label with interim data readouts 3,4 within 15 years of diagnosis • SC dosing with duration of
treatment TBD (prior regulatory discussions IgA Nephropathy (IgAN) support up to 24 weeks) 5,6 • Key assessments: Drug localization and impact in tissue, biomarkers Up to 40% develop ESRD w/in 20 years of diagnosis , and patients 7,8
(including surrogate endpoint biomarkers proteinuria and eGFR) for have 10 years reduced life expectancy assessment of ADX-097 activity 5,9 ~70% not adequately controlled w/supportive care • Anticipated to provide data for key regulatory
discussions C3 glomerulopathy (C3G) Trial initiated; topline results expected in 2H’25, with initial open-label Up to 50% of adult, 70% of pediatric patients progress to kidney failure 10-13 data by 1H’25 within 10 years >70%
experience recurring disease; ~50% experience allograft loss w/in 10 10,14-17 years of kidney transplant 1. Mahajan et al. Lupus 2020; 2. Cervera et al. Medicine 2002; 3. Maroz et al. Am J Med Sci 2013. 4. Ward et al. J Rheumatol 2009; 5. Habas et
al. Medicine (Baltimore) 2022. 6. Berthoux et al. Semin Nephrol 2008; 7. Pitcher et al. Clin Jour of Amer Soc Neph 2023. 8. Hastings et al. Kidney Int Rep 2018; 9. Raun et al. N Engl J Med 2015; 10. Heiderscheit et al. Am J Med Genet C Semin Med
Genet 2022. 11. Smith et al. J Am Soc Nephrol 2007; 12. Servais 32 et al. Kidney Int 2012; 13. Rabasco et al. Kidney Int 2015; 14. Smith et al. Nat Rev Nephrol 2019. 15. Welte et al. BMC Nephrology 2018; 16. Salvadori et al. WJT 2016. 17.
Regunathan-Shenk et al. AJKD 2019 18. Hoover et al. Kidney Int 2016; 19. Pryor et al. Rheum Dis Clin North Am. 2021; 20. Braun et al. Int Urol Nephrol 2011; 21. McQuarry et al. Kidney Int 2013; 22. Bomback et al. Kidney Int. 2018.
Q32 Bio Has Significant Potential to Unlock Near-term Value-creation
Runway through multiple Phase 2 clinical readouts and into mid-2026 Financial • Q3 cash balance of $89.1M, providing expected cash runway to mid 2026 Overview • Approximately 12.1M shares outstanding • 1H25: Bempikibart AA Ph2 Part
B initiation Numerous Anticipated • 1H25: Renal basket Ph2 initial data Milestones in 2025 • 2H25: Renal basket Ph2 topline results 33

APPENDIX
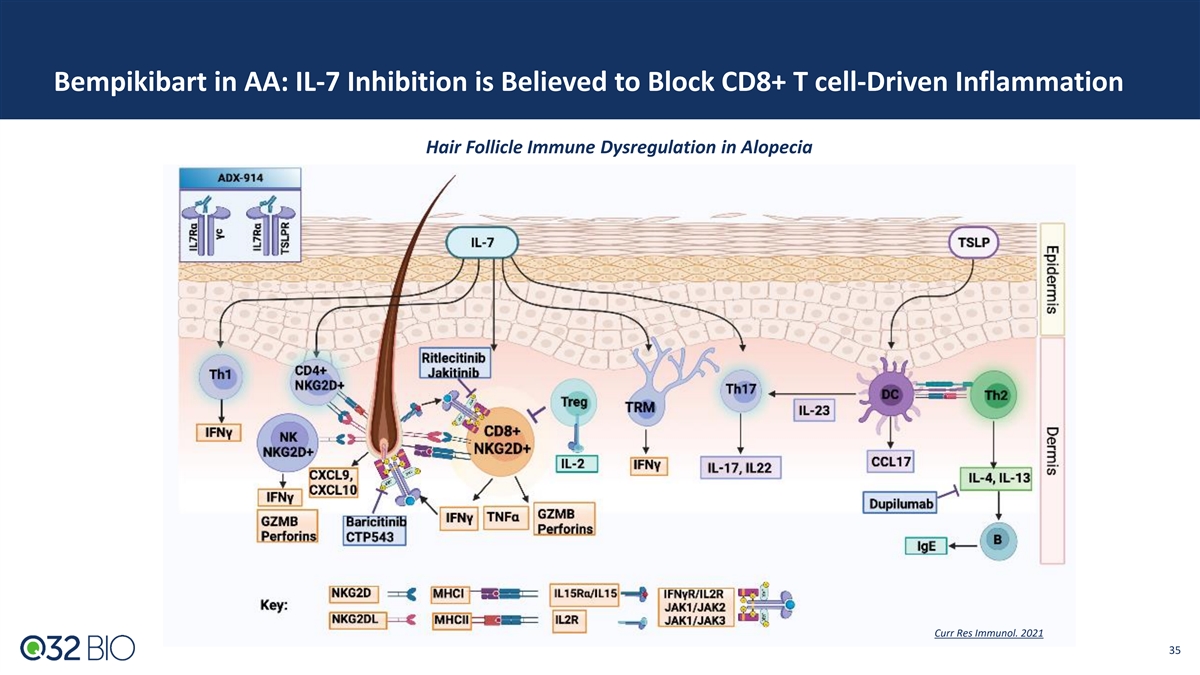
Bempikibart in AA: IL-7 Inhibition is Believed to Block CD8+ T
cell-Driven Inflammation Hair Follicle Immune Dysregulation in Alopecia Curr Res Immunol. 2021 35
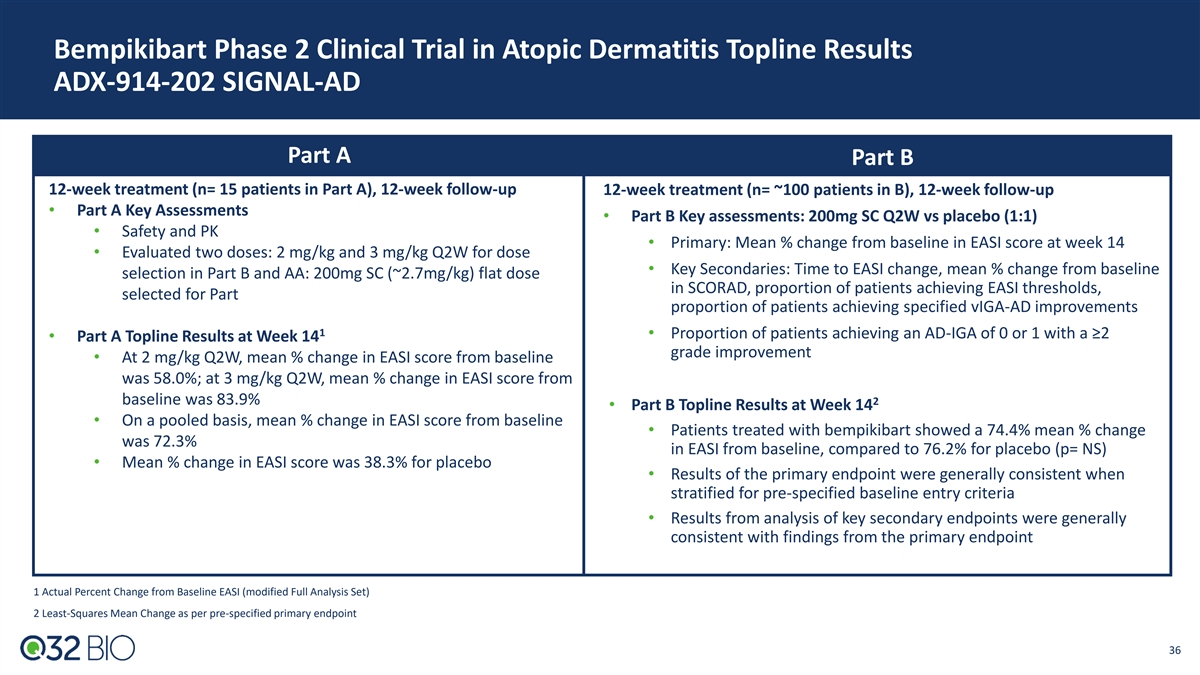
Bempikibart Phase 2 Clinical Trial in Atopic Dermatitis Topline Results
ADX-914-202 SIGNAL-AD Part A Part B 12-week treatment (n= 15 patients in Part A), 12-week follow-up 12-week treatment (n= ~100 patients in B), 12-week follow-up • Part A Key Assessments • Part B Key assessments: 200mg SC Q2W vs placebo
(1:1) • Safety and PK • Primary: Mean % change from baseline in EASI score at week 14 • Evaluated two doses: 2 mg/kg and 3 mg/kg Q2W for dose • Key Secondaries: Time to EASI change, mean % change from baseline selection in
Part B and AA: 200mg SC (~2.7mg/kg) flat dose in SCORAD, proportion of patients achieving EASI thresholds, selected for Part proportion of patients achieving specified vIGA-AD improvements 1 • Proportion of patients achieving an AD-IGA of 0 or
1 with a ≥2 • Part A Topline Results at Week 14 grade improvement • At 2 mg/kg Q2W, mean % change in EASI score from baseline was 58.0%; at 3 mg/kg Q2W, mean % change in EASI score from baseline was 83.9% 2 • Part B Topline
Results at Week 14 • On a pooled basis, mean % change in EASI score from baseline • Patients treated with bempikibart showed a 74.4% mean % change was 72.3% in EASI from baseline, compared to 76.2% for placebo (p= NS) • Mean %
change in EASI score was 38.3% for placebo • Results of the primary endpoint were generally consistent when stratified for pre-specified baseline entry criteria • Results from analysis of key secondary endpoints were generally consistent
with findings from the primary endpoint 1 Actual Percent Change from Baseline EASI (modified Full Analysis Set) 2 Least-Squares Mean Change as per pre-specified primary endpoint 36
v3.24.3
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14a
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
Q32 Bio (NASDAQ:QTTB)
Historical Stock Chart
From Nov 2024 to Dec 2024

Q32 Bio (NASDAQ:QTTB)
Historical Stock Chart
From Dec 2023 to Dec 2024

